
Critical Update: How to Optimally Rotate the Pelvis during the Downswing
Click here to go back to the homepage.
Introduction:
In this review paper I will be detailing in considerable depth my updated
opinions regarding the optimal method of performing a rotary pelvic motion
during the downswing. I will specifically describe in great detail the anatomy
of the pelvis and pelvic girdle muscles, and the likely biomechanical actions
used by many professional golfers when they rotate their pelvis during their
downswing action. I will not be originating any "new" methods on how best to
perform the rotary motion of the pelvis during the downswing action, because the
world's greatest professional golfers already know how to optimally perform a
rotary pelvic motion during their downswing action, and I am merely presenting
my "beliefs/opinions" regarding the fundamental biomechanics that I believe they use when
they perform their rotary pelvic motion. I suspect that many modern-day golf instructors are
teaching a suboptimal pelvic motion technique and I also believe that many
amateur golfers are using the wrong muscles to perform a rotary pelvic motion
during their early-mid downswing. I think that those amateur golfers could
significantly improve their rotary pelvic motion during the downswing if they
would use the same pelvic motion biomechanics that are used by many professional
golfers (like Sam Snead, Ben Hogan, Jack Nicklaus, Arnold Palmer, Lew Worsham,
Jordan Spieth and Jason Day) and I hope that this review paper will provide
those amateur golfers with a much greater insight into the optimum way of
performing a rotary pelvic motion during the downswing.
I have produced a 1 hour 48 minute video to supplement this review paper, and I have posted that video on you-tube.
https://www.youtube.com/watch?v=bByKt7LRP2g
In that *video I demonstrate many of the same fundamental principles that I discuss in this review paper, and I hope that the supplementary video will help interested readers better understand my opinions regarding the biomechanics of the "rotary pelvic motion during the backswing and downswing".
(* Note that I frequently/mistakenly referred to the greater trochanter as the greater tuberosity, and the lesser trochanter as the lesser tuberosity during my unedited/extemporaneous video presentation, and I occasionally mixed up words eg. using the word "left" when I obviously meant "right". Also, note that I am an inflexible 67 year old senior golfer who lacks the ability to demonstrate the rotary pelvic motions efficiently, so always remember to listen to what I am saying if my body motions are not condordant with I am saying at any time point during the video presentation)
Finally, note that I previously wrote a review paper regarding the topic of pelvic motion during the downswing - The Backswing and Downswing Hip Pivot Movements: Their Critical Role in the Golf Swing - but I now regard my personal opinions expressed in that review paper as being oversimplistic and outdated, and they no longer represent my personal point of view. My personal opinions expressed in this review paper more accurately represent my present-day's (much more refined) thinking regarding the rotary pelvic motion that happens during a professional golfer's downswing.
Explaining the anatomy and biomechanics of an optimal rotary pelvic motion during the backswing and downswing
To perform a high quality golf swing at a professional level, I believe that a golfer should use an active pivot action type of golf swing where the active pivot action essentially powers the golf swing (via the pivot-induced release of PA#4). The pivot action can be thought of as a sequential kinematic phenomenon where the lower body (pelvis) rotates first, and the upper torso rotates secondarily after a variable degree of time delay. Any degree of time delay may produce a finite degree of dynamic X factor stretching of the upper torso's musculature (which some golfers believe is biomechanically advantageous) and it obviously creates a greater amount of torso-pelvic separation during the transition to the downswing. The start of the counterclockwise pelvic rotation may begin in the late backswing (eg. between P3.75 and P4) or it may only start at the P4 position (defined as the moment that the club suddenly changes direction). I believe that a characteristic biomechanical feature of a good quality pivot action is that it is fundamentally a rotary motion of the torso that happens between the feet, and there should be no side-to-side swaying motion of the torso that moves the body beyond the lateral boundaries of the feet. A *small degree of left-lateral pelvic shift is acceptable during the early downswing, but the downswing motion of the pelvis should primarily be thought of as being rotary in nature.
(* I will describe a number of factors that determine the amount of left-lateral pelvic shift that can occur during the early downswing later in this review paper).
Consider an example of a golfer who perfectly exemplifies the rotary motion of the torso that should happen in a good quality, professional golf swing.
Back view video of Jamie Sadlowski's golf swing - https://www.youtube.com/watch?v=5gekd_JMFT4
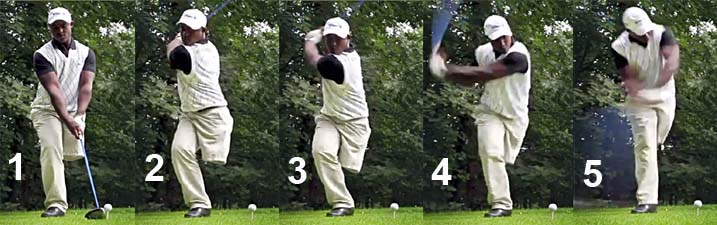
Here are capture images of Jamie Sadlowski's downswing action.
Image 1 shows Jamie Sadlowski at his end-backswing position (P4 position). Note that he rotated his pelvis about 50-60 degrees clockwise during his backswing, but he rotated his upper torso (shoulders) much more than he rotated his pelvis thereby generating a finite amount of static X factor (torso-pelvic separation). Note that his pelvis and upper torso are centralised between his feet, and there is no evidence of any side-to-side swaying motion of his torso.
Image 2 shows his early downswing action which starts off with a counterclockwise rotation of his pelvis that automatically/naturally causes the lumbar spine to rotate counterclockwise to roughly the same degree. His upper torso starts to rotate momentarily later and it involves a counterclockwise rotation of the thoracic spine. Note how his pelvis and upper torso remain centralised between his feet and there is no evidence of any deliberate weight-shift during his early downswing action.
Image 3 is at the P5.5 mid-downswing position. Note that his pelvis still leads the upper torso from a rotary perspective and that his pelvis is more open than his upper torso (thorax) - and that allows him to more easily acquire secondary axis tilt and right lateral bend, that in turn makes it easier for him to slot his power package in an "in-to-out" manner and thereby avoid any roundhousing motion of his upper torso and arms.
Image 4 is at impact. Note that his pelvis is more open than his upper torso. Note that both his pelvis and upper torso are still roughly centralised between his feet and there is no evidence of any overt swaying motion of his torso in a targetwards direction during his entire downswing action.
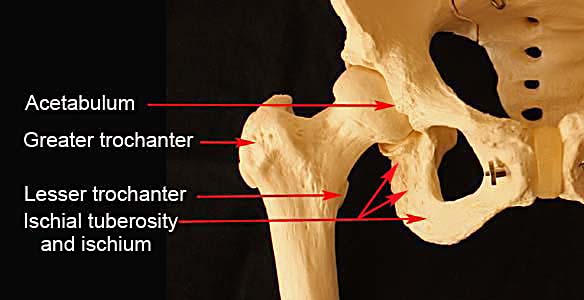
Before I continue to discuss the biomechanics underlying the rotary motion of the pelvis during the downswing, I will first point out certain anatomical features of the pelvis.
Consider two photographic images that I took of a plastic cast-model of the human pelvis.
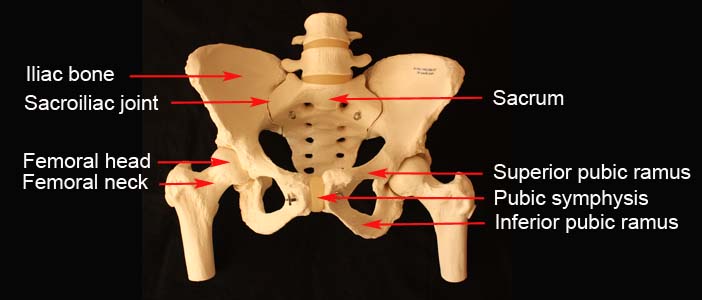
The pelvis can be thought of as basically consisting of two skeletal
half-structures (with each half consisting of iliac, pubic and ischial bony
subsections) that are conjoined together at the back by the sacrum (at the left
and right sacroiliac joints) and at the front by the ligamentous pubic symphysis (which can
be thought of as being equivalent to a joint). Because the sacro-iliac joints
and pubic symphysis are only lax during late pregnancy, it is useful to think of
the entire pelvis and sacrum as being an unitary bony (skeletal) structure that
can only rotate as a single rotating skeletal entity, which means that the left
side of the bony pelvis cannot rotate more (or less) than the right side of the
bony pelvis. Now, although the left half of the bony pelvis cannot rotate more
(or less) than the right half of the bony pelvis from an intrinsic skeletal
perspective, it is possible for the right half of the lower body (pelvis) to
rotate more (or less) than the left half of the lower body (pelvis) if one views
the rotational motion of the lower body (pelvis) from an extrinsic perspective - and what
makes this phenomenon biomechanically possible is that the pelvis has no single
axis of rotation that is centrally located. Any rotary motion of the pelvis
during the golf swing action occurs due
to joint motion happening at the level of the two hip joints, and it is
biomechanically possible for there to be more translational and rotational
motion happening at one of the hip joints (relative to the opposite hip joint)
because of the presence of biomechanical factors that affect each hip joint's resistance/impedance to
any translational (or rotational) motion happening at the level of each
hip joint.
Consider this cardboard cut-out that is shaped to resemble the oval shape of a human pelvis.
Capture image from my video presentation.
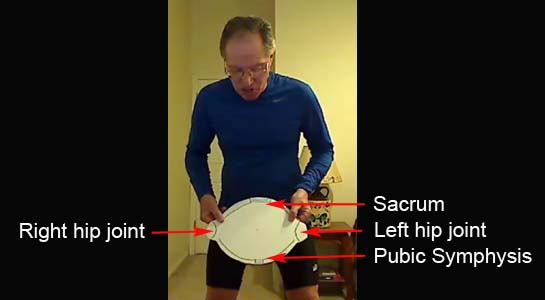
Note that I am holding a piece of cardboard that has been shaped to resemble the oval-shaped human pelvis with two hip joints at opposite ends.
Now imagine what would happen if it were possible to create a humanoid robot that only had a single supporting leg that articulated with the pelvis centrally, so that the pelvis could rotate around the single/central vertical axis of that centralised leg.

In this demonstration (from my video), I have placed a bicycle spoke through a hole in the center of the cardboard pelvis, and that bicycle spoke represents a single/central pelvic axis around which the pelvis can rotate. Note that the bicycle spoke is being held perpendicular to the inclined plane (swingplane).
Image 1 shows the orientation of the pelvis at address, where the pelvis is square to the target, and where an imaginary horizontal line drawn between the two hip joints is parallel to the ball-target line (which is the base of the inclined plane). R1 represents the position of the right hip joint at address, and L1 represents the position of the left hip joint at address.
Image 2 shows what would happen if I rotate the pelvis clockwise by ~50 degrees in the direction of the curved red arrow (mimicing the pelvic rotation in the backswing). The right hip joint will move to position R2. While that is happening, the left hip joint will move in the direction of the curved blue arrow to position L2. The amount of movement of the left hip joint will be identical to the amount of movement of the right hip joint because the rotation of the pelvis is happening symmetrically around a single/centralised axis through the middle of the pelvis.
Image 3 shows what would happen if I rotate the pelvis counterclockwise so that the right hip joint moves from the R2 position to the R3 position (mimicing the pelvic rotation during the early downswing) - the left hip joint will move symmetrically by exactly the same amount from position L2 to position L3.
In other words, the two hip joints always move symmetrically by exactly the same amount during any clockwise (or counterclockwise) rotation of the pelvis.
As I previously stated, this phenomenon of a symmetrical rotational motion of the two hip joints doesn't necessarily happen in a "real life" golfer's golf swing action because there is no single/central axis of rotation. In a "real life" professional golfer who performs a rotary pelvic motion during the backswing/downswing, the pelvis rotates because of 3-D translational/rotational movements of the two femoral heads in 3-D space.
Consider the average amount of pelvic rotation that may occur in a skilled golfer's full golf swing action.

Image 1 represents the address position where the pelvis is square to the target, and where the horizontal pelvic axis between the two hip joints is parallel to the ball-target line (base of the inclined plane).
Image 2 shows the end-backswing position of the pelvis if it rotates clockwise by ~50 degrees during the backswing action.
Image 3 shows the pelvis at the end of the "hip-squaring phase" (which usually happens by P5) and note that the pelvis is again square having rotated counterclockwise by ~50 degrees during the early downswing.
Image 4 shows an open pelvis at impact with the pelvis open by ~40 degrees.
The total amount of counterclockwise rotation of the pelvis happening in the downswing is ~90 degrees. Note that the left hip joint has rotated counterclockwise by ~90 degrees during the downswing and this represents the "left hip clearing" action where the left hip joint rotates counterclockwise away from the ball-target line in the direction of the tush line (which is an imaginary line drawn against the back of the right buttocks at the P4 position) during the downswing action. Note that according to my arbitrary definition of the *"left hip clearing" action, it starts at P4 and ends at impact, and it consists of two rotational phases - i) phase 1 is the "hip-squaring phase" that happens between P4 and P5 and ii) phase 2 happens between P5 and impact. I have arbitrarily divided the "left hip clearing" action (which is really a continuous/non-interrupted rotary motion) into those two phases because I believe that different pelvic girdle muscles and different biomechanical actions are used to rotate the pelvis in phase 1 (compared to phase 2).
(* Many golf instructors talk of the "left hip clearing action" in a very different manner, and they refer to the "left hip clearing action" as happening in the later downswing and they believe that the pelvis must first shift left-laterally towards the target in the early downswing before one can perform the counterclockwise rotational pelvic motion [that represents a "left hip-clearing action" where the left hip joint area of the left pelvis rotates back towards the tush line]. I believe that it is fundamentally incorrect to believe that it is mandatory to shift the pelvis left-laterally [in order to first get the left leg weight-pressure loaded] before one initiates the counterclockwise rotation of the pelvis and I will provide many pro golfer-examples of how the pelvis starts to rotate counterclockwise from the very start of the downswing without any need for a mandatory/preliminary weight-shift of the pelvis in a targetwards direction.)
Now, consider three different rotary-translational pelvic motion patterns that can happen in the early downswing (during the hip-squaring phase of the "left hip clearing" action).
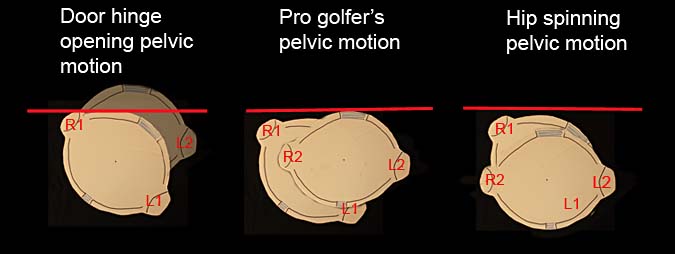
I have used Photoshop to produce two images of the cardboard pelvis in each of the three pelvic motional patterns - the one image shows the pelvis at the P4 position (R1 being the position of the right hip joint and L1 being the position of the left hip joint) and the second image shows the pelvis at the end of the hip-squaring phase, which usually happens at/near the P5 position (R2 being the position of the right hip joint and L2 being the position of the left hip joint). The red line represents the tush line (imaginary line drawn against the back of the right buttocks at the P4 position).
Now, consider the first pelvic motional pattern - the door hinge opening type of pelvic motional pattern. In this type of pelvic motional pattern, note that the right hip joint remains in roughly the same location during the early downswing between P4 and P5, while the left hip joint gets pulled back towards the tush line to such a large degree that the back of the left buttock gets pulled back beyond the tush line by the end of the hip-squaring phase. In this particular type of "left hip clearing action" pattern, there is no lateral shift of the pelvis towards the target and the left hip joint simply gets pulled back towards the tush line during the "left hip clearing action" (like a door opening). The right hip joint can be considered to be equivalent to a "fixed" door hinge, which doesn't move its position while the door is opening. That's why I have arbitrarily labelled this type of pelvic motional pattern a "door hinge opening" type of pelvic motion.
Consider a golfer who manifests this "door hinge opening" type of pelvic motion pattern.
Manuel De Los Santos swing video - https://www.youtube.com/watch?v=aw-nt0eTb2w
Here are capture images from the swing video showing his downswing action
Note that Manuel De Los Santos has his left thigh amputated at the level of his
mid-thigh and he pivots over only one leg (right leg) during his downswing.
Image 1 shows Manuel De Los Santos at the address position with his pelvis square to the ball-target line.
Image 2 shows Manuel De Los Santos at his end-backswing position. Note that he has "turned into" his right hip joint during his backswing so that his right hip joint is in a state of internal rotation at the P4 position (due to the fact that he has rotated his pelvis more clockwise than he has rotated his right thigh). Note that his upper left thigh is hanging limply in a state of external rotation at the level of the left hip joint.
Image 3 shows how he starts to rotate his pelvis counterclockwise at the very start of his downswing and he is pulling his left buttocks (and left hip joint) back towards the tush line in an overt "left hip clearing action" manner.
Image 4 shows him at the end of the hip squaring phase, which happens slightly before he even reaches the P5 position. Note how far he has pulled his left buttocks (left hip joint) away from the ball-target line in the direction of the tush line and note that the back of his left buttock has even got further back than the tush line. Note that his right hip joint has not moved left-laterally towards the target, and it has only moved vertically upwards to a small degree as he slightly straightens his right thigh between P4.5 and P5.
Note that Manuel De Los Santos can perform a perfectly executed "left hip clearing action" without first shifting his weight left-laterally onto his left foot (which is non-existent). His downswing's pelvic motional pattern demonstrates that it is a fallacy to believe that a golfer must first shift the pelvis left-laterally in a weight-shifting manner before he performs a "left hip clearing action". In fact, it is biomechanically much easier for a two-legged golfer to externally rotate the left femur and withdraw the left hip joint in a "left hip clearing action" manner when the left leg is not significantly weight-pressure loaded than when it is more weight-pressure loaded. In a two-legged golfer, the average "COP-measurement under the left foot at P4 is 20-30% of the overall COP-measurement, while it is 50% of the overall COP-measurement at P5.
(*COP = center of pressure, and its measurement, using force plate technology, is a quantitative method of measuring the weight-pressure loading of the two feet at all times during the golf swing action, and the COP-measurement under each foot is usually expressed as a percentage of the overall COP-measurement)
Now, consider the second pelvic motional pattern - which I have arbitrarily labelled a "pro golfer's pelvic motion" pattern.
The pro golfer's pelvic motion pattern is used by the majority of professional golfers and it has the following characteristics. During the hip-squaring phase, the right hip joint remains nearly in the same location and it only moves a few inches in a targetwards and outwards direction, while the left hip joint moves much more in space and it mainly moves backwards in a direction that is away from the ball-target line and towards the tush line. There is very little (only 1-3") of left-lateral pelvic shift happening during this first phase of the "left hip clearing action" and there should be no deliberate attempt to shift one's body weight targetwards. Note that the back of the right buttock (or sacrum) remains at, or very near, the tush line during the entire duration of the early downswing between P4 and P5.
Consider a few golfer-examples who manifest this pattern.
Jamie Sadlowski
Here are capture images from a DTL video of Jamie Sadlowski's swing.
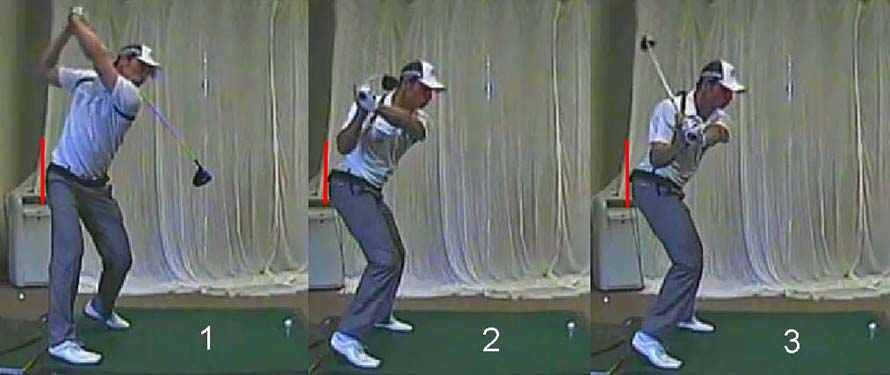
Image 1 shows Jamie Sadlowski at his P4 position. I have drawn a red line against the back of his right buttock at his end-backswing position and that red line represents the tush line.
Image 2 shows Jamie Sadlowski at the P4.5 postion and image 3 shows him at the P5 position (end of the hip squaring phase). Note how much Jamie Sadlowski has pulled his left hip joint (left buttock) back toward the tush line while still keeping his right buttock close to the tush line, thereby avoiding any premature outward motion of his right hip joint in the direction of the ball-target line.
Consider face-on capture images of Jamie Sadlowski's early downswing action.

Image 1 is at P4 and image 5 is at P5. Note that he has a square pelvis at the
P5 position and both femurs are in a state of symmetrical external rotation at the
level of their respective hip joints, and he is therefore prototypically
manifesting the Sam Snead "sit-down" look. Note that his pelvis remains
centralised during his early downswing and there is minimal left-lateral pelvic
shift happening during the first phase of his "left hip clearing action". Note
that Jamie Sadlowksi does not "appear" to be shifting his body weight
left-laterally in a targetwards direction while he performs his rotary type of
pivot action (where he first rotates his pelvis counterclockwise, followed
shortly thereafter by a counterclockwise rotation of his upper torso around his
rightwards-tilted thoracic spine).
Jack Nicklaus
Birds-eye swing video of Jack Nicklaus and other professional golfers - https://www.youtube.com/watch?v=StKkT9sTTtQ
Here are capture images of Jack Nicklaus' early downswing.

Image 1 shows Jack Nicklaus at his end-backswing position. I have drawn a red
line against the back of his right buttocks, and that red line represents the
tush line.
Image 2 shows Jack Nicklaus at P4.5 and image 3 shows Jack Nicklaus at the end of his hip-squaring phase (P5 position). Note how much he has pulled his left buttock back towards the tush line, while still keeping his right buttock against the tush line, during his early downswing's P4 => P5 time period.
Note that there is minimal left-lateral pelvic shift happening during his hip-squaring phase.
Birds-eye view swing videos are particularly useful in studying the movement of the right buttock away from the tush line in the early downswing, and here are capture images from another good quality birds-eye view swing video - featuring a student-golfer of Geoff Jones (aka Slicefixer).

Image 1 shows the student-golfer at his end-backswing position. I have drawn a
red line against the back of the right buttock, and that red line represents the
tush line.
Image 2 shows the student-golfer at the P5 position - at the end of his hip-squaring phase. Note how much he has pulled his left buttock (and therefore his left hip joint) back towards the tush line, while still keeping the back of his right buttock against the tush line.
Note that his pelvis has moved a few inches left-laterally during his hip-squaring action, which means that the right hip joint has moved targetwards to a small degree. However, note that his right hip joint is not prematurely moving outwards (towards the ball-target line) in a hip-spinning manner between P4 and P5.
I will shortly describe the biomechanics that underlie a pro golfer's pelvic motion pattern in great detail, but first consider the third pelvic motion pattern - the hip spinning pelvic motion pattern.
In the hip spinning pelvic motion pattern, the right hip joint
immediately moves outwards in the direction of the ball-target line, and the
right buttock therefore immediately leaves the tush line, at the very start of
the downswing. By contrast, the left hip joint doesn't move very much backwards
away from the ball-target line (towards the tush line) during that same time
period. At the end of the hip
squaring phase, both the left and right buttocks are many inches away from the
tush line. I regard the hip spinning pelvic motion pattern as being a suboptimal method
of rotating the pelvis during the downswing and I will describe the underlying causal biomechanics later in this review
paper.
Biomechanics underlying the performance of a pro golfer's pelvic motion pattern
I believe that this type of pelvic motion pattern is the
optimal method of rotating the pelvis in the early downswing between P4 and P5,
and I will describe the underlying biomechanics in great detail.
I believe that the key muscles used to perform this type of rotary pelvic motion are the right-sided and left-sided lateral pelvic rotator muscles, and it is important to understand how contraction of those muscles cause a counterclockwise rotation of the pelvis at the start of the downswing.
Here is a capture image (from that video) showing the 6 lateral pelvic rotator muscles.
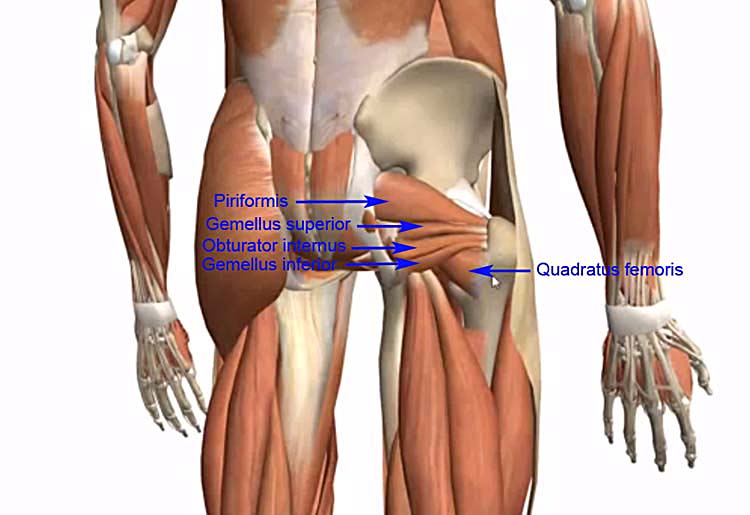
I have pointed out the i) piriformis muscle, the
ii) gemellus superior
muscle, the iii) gemellus inferior muscle, the iv) obturator internus muscle, and
the v) quadratus femoris muscle. The vi) obturator externus muscle cannot be
seen from this viewing perspective because it is hidden beneath the
overlying lateral pelvic rotator muscles.
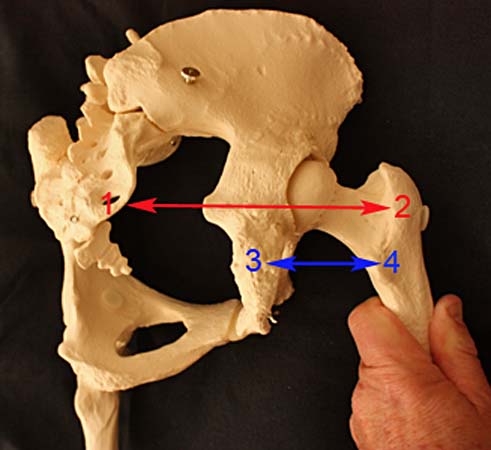
Note that I rotated the pelvis about 50 degrees clockwise before I took
this photograph of my plaster-cast pelvic model. Note that I have
prevented the right femur from rotating clockwise by the same amount, so
that the right femur becomes internally rotated in the
right hip joint. When the right femur is internally rotated in the right
hip joint, that means
that the points of insertion of the lateral pelvic
rotator muscles (points 2 and 4) are further away from their
points of origin (points 1 and 3). The points 1 - 2
represent the points of origin and insertion of the piriformis muscle and the points 3 - 4 represent the
points of origin and insertion of the quadratus femoris muscle. I have only referred to those two lateral
pelvic rotator muscles as representative examples, but all the 6 lateral
pelvic rotator muscles on the right side are similarly stretched at the
end-backswing position when the right femur is internally rotated in the
right hip joint.
When the 6 right-sided lateral pelvic rotator muscles are stretched at the end-backswing position, they are ready to contract during the early downswing. If they contract and shorten (thereby decreasing the distance between their points of origin and their points of insertion) they can cause external rotation of the right femur in the right hip joint if the pelvis is stabilised or a counterclockwise rotation of the pelvis away from the right femur if the right femur is stabilised. This is a critical point that one needs to fully understand - so I will discuss this issue in greater detail.
I stated that if
Here is a
link to pages from the online version of that textbook.
Read pages 277- 279.
If you decide not to read those pages, here are the relevant sections in an excerpted form.
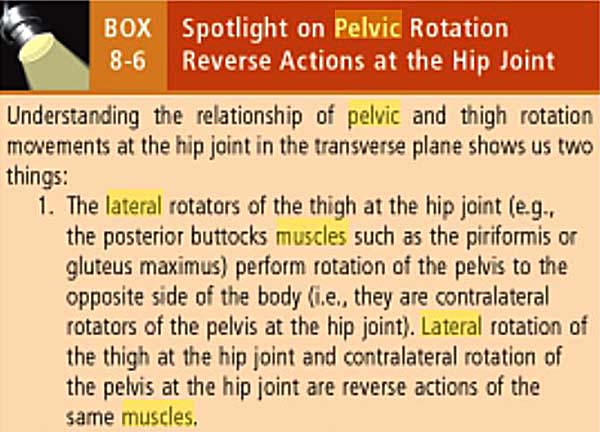
Note that the author states that the lateral pelvic rotator muscles can cause lateral (external) rotation of the thigh at the level of the hip joint and also a contralateral rotation of the pelvis at the hip joint, and that these two motions are merely reverse actions of the same muscles.
Now, consider those differential (reverse) actions in diagrammatic form.
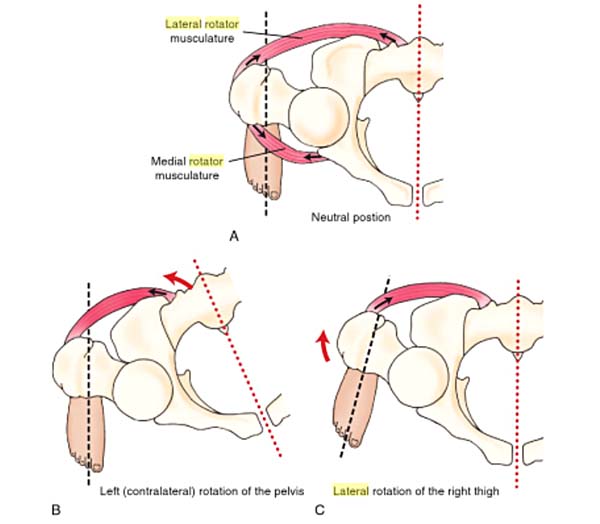
Diagram A shows the pelvis and ipsilateral femur in a neutral position.
The black arrows shows that if the muscles contract and shorten, that
they will cause the muscle's origin (on the pelvis or sacrum) and
the muscle's insertion (on the upper femur) to move closer towards each
other. Diagram B shows that if the right femur is "stabilised" that contraction
of the right-sided lateral pelvic rotator muscles will cause the pelvis to
rotate counterclockwise away from the "stabilised" right femur. Diagram C shows
that if the pelvis is "stabilised" that contraction of the right-sided lateral
pelvic rotator muscles will cause the right femur to laterally (externally)
rotate in the right hip joint. I believe that diagram B is very applicable to
the right hip joint/femur between P4 and P4.5 if weight-pressure loading of the right leg (due to the golfer
actively pushing down into the ground under the right foot) causes the right
leg to become "stabilised". At the end-backswing position, a pro golfer
has roughly 70-80% of his overall COP-measurement under his right foot and if he
maintains, or even slightly increases, his degree of weight-pressure loading of
his right leg/foot at the start of the early downswing, he can very effectively
stabilise the position of the right femur is space. Then, when the right-sided
lateral pelvic rotator muscles contract, they will cause a counterclockwise
rotation of the pelvis away from the "stabilised" right femur.
Consider a similar type of scenario from my video presentation - featuring the contraction of the triceps muscle that causes the elbow joint to straighten (extend).
Capture images from my video presentation.

In images 1 and 2, I am demonstrating how contraction of the right triceps
muscle causes straightening (extension) of the right elbow. In image 1, I had
previously contracted my right biceps muscle to flex my right elbow, while
simultaneously stretching my passively relaxed right triceps muscle, and that
particular muscle action brought my right hand closer to my right shoulder
socket.
In image 2, I contracted (and shortened) the right triceps muscle and that caused my right hand to move further away from my right shoulder socket as my right elbow straightened (extended). Why did my right hand move away from the right shoulder socket, rather than my right shoulder socket move away from my right hand? The answer is obvious - the biomechanical resistance (impedance) that my right hand presents to any move away from the right shoulder socket is far less than the biomechanical resistance (impedance) that my right shoulder socket (and the conjoined upper torso) presents to any move away from my right hand because my right hand is freely mobile in space and it can be easily moved (with very little triceps muscle contractile force required to straighten my right elbow).
Now, consider a scenario where I am positioned closer to the wall with the base of the palm of my right hand barely touching the wall - see image 3.
When I contract my right triceps muscle, it cannot cause my right hand to move further away from my right shoulder socket because the wall offers too much resistance (impedance). Therefore, an isotonic contraction of my right triceps muscle will cause my right shoulder socket (and conjoined upper torso) to move away from my right hand, which can be deemed to be "stabilised" by the presence of the wall resisting any push-force that is being applied against the wall - see image 4. As the right triceps muscle starts to isometrically contract it will start to generate a muscle-derived "action force" that pushes my right palm against the wall with a progessively increasing force, and that will produce a sensory "feeling of pressure" being felt under the base of my right palm where it abuts against the wall. That "feeling of pressure" will increase until the right triceps muscle has produced enough isometric contractile force to move the right shoulder socket (and my conjoined upper torso) away from my "stabilised" right hand. When my right elbow eventually straightens due to the isotonic contraction of my right triceps muscle, I will "feel" progressively less pressure-sensation under the base of my right palm where it abuts against the wall. It is important to realize that the wall is not the primary causal agent that is causally producing the "feeling of pressure" under my right palm and any pressure-sensation that I experience under my right palm is primarily due to an "action force" involving a muscular contraction of the right triceps muscle, and the "reaction force" is secondarily produced by the wall resisting any push-force produced by my right palm against the wall. From a "cause-and-effect" perspective, it is the contraction of my right triceps muscle that is the inciting causal agent that secondarily generates a Newtonian type of "reaction force" due to the wall resisting any push-force being applied by the palm of my right hand against the wall.
So, getting back to the start of the downswing where a pro golfer "stabilises" his right leg/foot by pressing down into the ground, an "action force" is being directed vertically downwards secondary to the contraction of muscles in the muscle zone of the right lower limb and right pelvic girdle, and that "action force" causes the right foot to move more firmly against the ground, while the "reaction force" is provided by the ground resisting the push-force exerted by the right foot against the ground. There is yet another "action force" and another "reaction' force" operant at the start of the downswing between P4 and P4.5 and those "forces" are shear forces operating in the horizontal plane under the right foot. If a professional golfer is analysed using force plate technology, that can measure both vertical and horizontal pressure-shear forces under the right foot at the start of the downswing, the force-pressure measurements in the horizontal plane are found to be directed clockwise under the right foot. It is as if the golfer is twisting his right foot clockwise (away from the target) against the resistance of the ground. What causes those shear forces to be detectably present under the right foot in the early downswing? I believe that they are likely to be secondary to the contraction of the right-sided lateral pelvic rotator muscles that attempt to rotate the right femur externally in the right hip joint. However, the pro golfer is resisting any rotary motion of his right femur by pushing downwards into the ground while simultaneously, but unconciously, twisting his right foot clockwise against the resistance of the ground. That muscle action (involving right-sided muscles of the right lower limb and lower body) "stabilises" the right leg/foot against the resistance of the ground and eventually results in the pelvis rotating away from the "stabilised" right leg/foot when the right-sided lateral pelvic rotator muscles start to isotonically contract. As the pelvis rotates counterclockwise away from the "stabilised" right leg/foot, the shear force measurement under the right foot will automatically/naturally decrease. The peak time period of the shear force, and the maximum amount of "shear force", experienced under the right foot will be measured just before the right-sided lateral pelvic rotator muscles start to isotonically contract (shorten) thereby rotating the pelvis away from the weight-pressure loaded right leg/foot and they will be maximally present when the right-sided lateral pelvic rotator muscles are generating their maximal amount of isometric contractile force. It is important to realise (from a causal perspective) that the "action force" is generated by the right-sided lateral pelvic rotator muscles and that the clockwise twisting shear force measured under the right foot (by a force-pressure plate) is secondarily due to a "reaction force" caused by the ground resisting any twisting of the right foot in a clockwise direction. From a "cause-and-effect" perspective, I think that it would be *incorrect to surmise that the simple biomechanical maneuver of twisting the right foot clockwise against the ground will cause the pelvis to rotate counterclockwise - if the right-sided lateral pelvic rotator muscles are not active.
(* I think that many golf instructors/ golfers get this "cause-and-effect" biomechanical relationship mixed-up and they incorrectly believe that the simple action of twisting the right foot clockwise against the resistance of the ground will cause ["trigger"] the pelvis to rotate counterclockwise, and they are totally unaware of the primary role of the right-sided lateral pelvic rotator muscles in this "cause-and-effect" scenario).
What role do the left-sided lateral pelvic rotator muscles play in rotating the pelvis counterclockwise during the P4 => P5 time period?
Consider the situation of the left hip joint at the end-backswing position if a golfer lifts his left heel during the backswing action and allows his left femur to be less externally rotated in the left hip joint (compared to the address position).
Capture images of Arnold Palmer from a swing video.
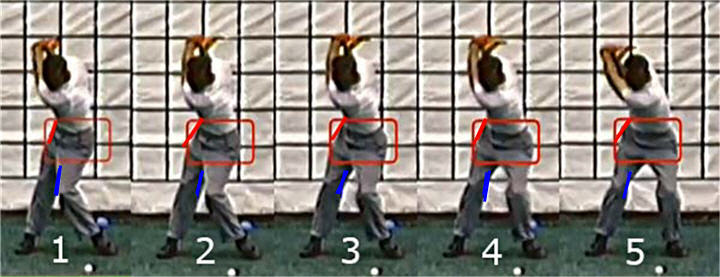
Image 1 shows Arnold Palmer at his end-backswing position. Note that his left knee is very close to his right knee due to the fact that he has adducted and internally rotated his left femur during his backswing action between P1 => P4. Note how much he has lifted his left heel off the ground, and that allows him to have a bent left knee at the P4 position with his left knee "pointing" at a spot behind the ball. Under those end-backswing conditions, the left-sided lateral pelvic rotator muscles are more passively stretched and ready to contract. Note that I have drawn a blue line against the inside of his left lower thigh/knee at his end-backswing position.
Image 2 shows his first move at the initiation of the downswing - which is a move of his left knee towards the target. Note that the targetwards motion of his left knee happens even before his pelvis seemingly starts to rotate counterclockwise. What causes his left knee to move targetwards? I believe that it due to activation of his left-sided lateral pelvic rotator muscles that externally rotate and abduct his left femur in his left hip joint. Why does activation of the left-sided lateral pelvic rotator muscles cause the left femur to externally rotate, rather than cause the pelvis to rotate clockwise away from the left femur? I believe that it is due to the fact that his left leg/foot is not weight-pressure loaded at his end-backswing position, which means that there is little impedance/resistance to external rotation of the left femoral head in the left hip joint when the left-sided lateral pelvic rotator muscles contract.
Note that his pelvis starts to rotate counterclockwise in images 3, 4 and 5 while his left knee continues to move targetwards. By the time he gets to the end of his hip-squaring phase (image 5), note that both thighs are are in a state of dual-external rotation in their respective hip joints.
Note how much his left knee has moved targetwards between image 1 => image 5 due to external rotation and abduction of his left femur in his left hip joint. However, that counterclockwise rotation of his left femur in his left hip joint - due to activation of his left-sided lateral pelvic rotator muscles - should theoretically not cause his pelvis to rotate counterclockwise. Nonetheless, there is another biomechanical action that is likely in play during the early downswing that enables the externally rotating left femur to assist in the counterclockwise rotation of the pelvis during the early downswing - and that biomechanical action is due to the simultaneous muscular contraction of the left adductor magnus muscle.
There has only been one electromyography study performed by golf researchers on pelvic girdle area muscles during a golf swing and that is the study by Bechler et al [1]. In that study, the golf researchers found that the lead adductor magnus muscle is very active during the early-mid downswing.
The adductor magnus muscle is the largest of the thigh adductor group of muscles and it has its origin on the inferior pubic ramus and it inserts on the medial (inner) surface of the lower-mid femur.
Here is a you-tube video showing the muscles in the medial compartment of the thigh - https://www.youtube.com/watch?v=ecfssWS1aVg
Here are capture images from the video showing the adductor magnus muscle.
Anterior (front) view

Note that I have yellow-highlighted the left adductor magnus muscle in that
image.
Posterior (back) view

During the early downswing between P4 and P5, the left femur is being externally
rotated due to contraction of the left-sided lateral pelvic rotator muscles so
that the left thigh becomes increasingly externally rotated at P5
(relative to the scenario at P4). However, if the the left adductor magnus is also isometrically active during this early
downswing time
period, it can pull the left inferior pubic ramus towards the left thigh (as it is being externally rotated),
thereby contributing to the counterclockwise rotation of the pelvis (which is
mainly due to contraction of the right-sided lateral pelvic rotator muscles). I
don't know how much the lead adductor magnus muscle contributes to the
counterclockwise rotation of the pelvis during the early downswing - compared to
the contribution from the right-sided lateral pelvic rotator muscles - but it
may play a significant role.
Now, consider another biomechanical phenomenon that is frequently (but not always) seen in professional golfers during the early downswing between P4 and P5 - and that biomechanical phenomenon is the increased degree of flexion happening at the level of the hip joints and knee joints.
Consider yet again these back-view images of Jamie Sadlowski's downswing action.
Image 1 shows Jamie Sadlowski at his end-backswing position - note that he has a
certain amount of flexion of his right hip joint and right knee joint.
Image 2 shows Jamie Sadlowski at the P4.5 position - note that he has an increased degree of flexion at the level of his right hip joint and right knee joint, and that causes his head to drop a few inches during his early downswing.
What is the relevance of this increased degree of hip joint and knee flexion that happens during the early downswing?
The first relevant benefit of increasing the degree of flexion of the right hip joint and right knee joint at the start of the transition to the downswing is that it allows a golfer to increasingly weight-pressure load, and thereby increasingly "stabilise", the right femur in space - so that the pelvis can be induced to more efficiently rotate counterclockwise AWAY from the increasingly "stabilised" right leg during the early downswing when the right-sided lateral pelvic rotator muscles contract (shorten).
The second benefit derived from increasing the degree of flexion at the level of the right hip joint is that it helps to ensure that the right femur externally rotates, and doesn't internally rotate, at the start of the downswing. Many unskilled amateur golfers start their downswing by "kicking-in" their right knee towards the ball and that biomechanical action would induce an adduction and internal rotation of the right femur. By contrast, most professional golfers keep their right femur externally rotated and slightly abducted during the early downswing's P4 => P5 time period, so that they acquire the Sam Snead "sit-down" look by the end of the early downswing (where both femur's are externally rotated in their respective hip joints by roughly the same amount).
Here is a diagrammatic image of Sam Snead as he gets near the P5 position (end of the hip-squaring phase).

Note that he looks like he is "squatting" and that both thighs are externally
rotated to the same degree - giving him the classic (prototypical) Sam Snead
"sit-down" look (as if he were starting to sit down on a bar stool).
Consider Jamie Sadlowski at the end of his hip-squaring phase.
Note that Jamie Sadlowski also has that "squatting" look at the end of his hip-squaring phase (image 5) where both femur's are externally rotated to roughly the same degree with respect to their respective hip joints, and he also prototypically manifests the Sam Snead "sit-down" look.
Note how much his head has dropped between his P4 position (image 1) and his P5 position (image 5), and note that it is primarily due to increased flexion at the level of his hip joints.
I previously stated that the second benefit derived from increasing the degree of flexion at the level of the right hip joint is that it helps to ensure that the right femur externally rotates, and doesn't internally rotate, at the start of the downswing. What is the underlying/explanatory biomechanical mechanism?
Consider the main pelvic girdle muscles that are causally responsible for increasing the degree of right hip joint flexion during the early downswing - the iliopsoas muscle (which is actually due to the combination of the iliacus muscle and the psoas major muscle).
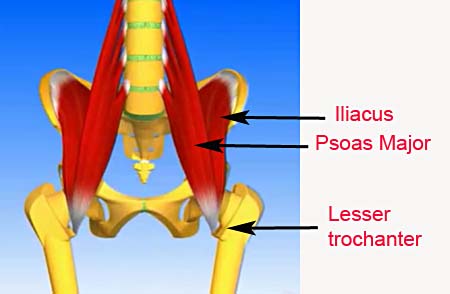
Note that the psoas major muscle has its origin on the lateral side of the upper
four lumbar vertebra while the iliacus muscle has its origin on the inner
surface of the iliac fossa. Both of those muscles join together to form a
conjoined tendon that inserts at the inner (medial) surface of the lesser
trochanter.
When the iliopsoas muscle contracts it shortens the distance between the lesser trochanter and the points of origin of the two muscles thereby causing increased flexion at the level of the ipsilateral hip joint.
However, because the point of insertion of the conjoined tendon at the lesser trochanter is on the inner (medial) side of the upper femur, it also causes external rotation of the ipsilateral femur when the iliopsoas muscle contracts - as demonstrated in the following image.

Note that when the right iliopsoas muscle contracts (see yellow arrow) it flexes the right thigh at the level of the right hip joint. However, note that it also simultaneously causes external rotation of the right femur (see curved white arrow, which demonstrates the counterclockwise rotation of the right femur).
That helps to explain why a skilled professional golfer
can routinely have his right femur in a state of external rotation at the level
of the right hip joint at the end of the hip-squaring phase - because the
external rotary torquing action of the right iliopsoas muscle supplements the
external rotary torquing action of the right-sided lateral pelvic rotator
muscles, which obviously promotes a state of external rotation of the right femur
in the right hip joint when the pelvis rotates counterclockwise
away from a "stabilised" right femur and "stabilised" right
foot (that is being torqued clockwise against the resistance of the ground due
to the external rotary torquing force). It is easy to understand
why the left femur is externally rotated at the end of the hip-squaring phase
because it is causally due to the contraction of the left-sided lateral pelvic
rotator muscles that externally rotate the left femoral head in the left hip
joint during the P4 => P5 time period. Remember that the left leg is not
weight-pressure loaded between P4 and P5, and only 20-30% of the overall
COP-measurement is located under the left foot at P4 and approximately 50% at P5
(which is the end of the hip-squaring phase). Therefore, there is no significant
impedance/resistance to external rotation of the left femur in the left hip
joint and it is biomechanically easy to ensure that the left femur is externally
rotated at the end of the hip-squaring phase.
Biomechanics of the pelvic motion in the mid-late
downswing between the P5 position and the P7 position (impact)
During the early downswing, the pelvis rotates about ~50 degrees counterclockwise (on average) and during that time period the pelvic crest remains roughly level relative to the ground, which means that the pelvis mainly rotates horizontally during the hip squaring phase.
During the mid-late downswing, the pelvis rotates another ~40 degrees counterclockwise (on average) which means that the pelvis would be ~40 degrees open at impact. Another biomechanical phenomenon that happens in the mid-late downswing is that the left pelvis elevates, so that it is higher than the right pelvis at impact.
Consider the muscle actions that are responsible for the horizontal and vertical motion of the pelvis during the mid-late downswing.
By the end of the hip-squaring phase, the lateral pelvic rotator muscles are significantly contracted (shortened) and they can no longer play a significant role in rotating the pelvis counterclockwise during the mid-late downswing. So, a relevant question arises-: Which muscles cause another 40 degrees of counterclockwise rotation of the pelvis during the 2nd phase of the "left hip clearing action" (during which time period the left hip joint moves increasingly towards the tush line in a counterclockwise rotary manner)? I believe that a few major muscles play an important role in causing the continued counterclockwise rotation of the pelvis during the mid-late downswing - the i) left knee extensors and ii) the left gluteus maximus muscle and the iii) left adductor magnus muscle.
Consider my biomechanical explanation.
A characteristic feature of a skilled professional golfer's late downswing action is the "fact" that the left leg progressively straightens due to extension at the level of both the left hip joint and the left knee joint while the left foot becomes increasingly weight-pressure loaded. At the P5 position (end of the hip-squaring phase) approximately 50% of the overall COP-measurement is located under the left foot, and this amount increases to approximately 80% of the overall COP-measurement by the P7 position (impact) in golfers (who are classified as "front foot" golfers).
Consider the implications of that "fact" by considering Ben Hogan's late downswing action (from a left back-viewing perspective).

Image 1 shows Ben Hogan at his end-backswing position and image 2 shows Ben
Hogan at the P5 position (end of the hip-squaring phase). Note that he manifests
the Sam Snead "sit-down" look at the P5 position - manifesting a significant amount of flexion at the
level of his left hip joint and left knee joint. Note that he pulled his left
buttocks back towards the tush line during his early downswing, and that
represents phase 1 of the "left hip clearing" action.
Image 4 shows Ben Hogan at impact. Note that his pelvis is about 40 degrees open at impact, which means that he rotated his pelvis another ~40 degrees counterclockwise during phase 2 of his "left hip clearing" action. A major factor that causes the left femoral head (and therefore the left hip joint) to move further back towards, and eventually back beyond, the tush line (and also more counterclockwise away from the target) during phase 2 of the "left hip clearing" action is the fact that the left leg is straightening, which means that the distance from the left foot to the left hip joint must increase. Because the left foot is solidly grounded during the later downswing as it is increasingly weight-pressure loaded (due to the fact that the COP-measurement under the left foot increases from 50% of the overall COP-measurment at P5 to 80% of the overall COP-measurement at impact), that means that the left femoral head (and therefore left hip joint) must move further away from the left foot and closer to the tush line during the left leg straightening action. Note how Ben Hogan's left knee becomes straightened (extended) at impact and that is due to the contraction of the left knee extensor muscles (especially the vastus lateralis muscle).
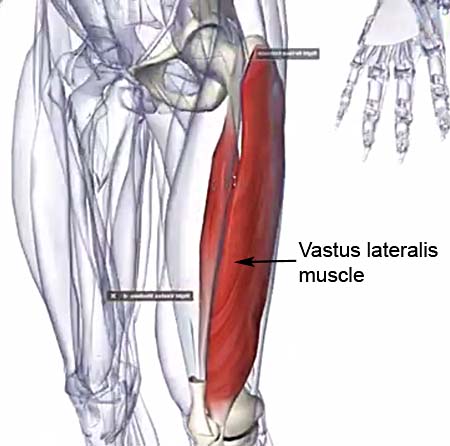
The left vastus lateralis muscle forms a large part of the left
quadriceps muscle group in the anterior compartment of the left thigh and when
it contracts it extends the left knee, and it also braces the left knee so that
it doesn't buckle/bend sideways (as evidenced in image 4 of the Ben Hogan downswing
series of capture images).
Another biomechanical factor that contributes to the continued counterclockwise rotation of the pelvis in the later downswing is the fact that the left adductor magnus muscle is still actively contracting and it pulls the left inferior pubic ramus (and therefore the left side of the lower pelvis) closer to the left femur. During the later downswing, the pelvis rotates counterclockwise more than the left femur, so that the left femur becomes progressively more internally rotated in the left hip joint, and isotonic contraction of the left adductor magnus muscle is continuously pulling the left femur and the left-lower pelvis closer together during this time period.
Also, note that Ben Hogan's left hip joint doesn't only move away from the ball-target
line, and therefore closer to the tush line, as he nears impact, it also moves
away from the target, and that is partly due to the active contraction of the left
gluteus maximus muscle.

The muscle lying under the black arrows is the left gluteus maximus
muscle, and it is attached medially (at its origin) to the outer (lateral) left edge of the sacrum and
to a significant section of the posterior pelvic crest and it inserts at the back of the upper
left femur. When that muscle contracts (and shortens in the direction of the
black arrows) it pulls the left upper femur towards the sacrum (midline) and
thereby contributes to the counterclockwise rotation of the left hip joint
away from the target as the left hip joint extends - see images 4 and 5
of the Ben Hogan downswing series of capture images.
During the impact and early followthrough time period, one often notes that a pro golfer's left femur externally rotates to a variable degree and that is also due to the continued isotonic contraction of the left gluteus maximus muscle. The reason why contraction of the left gluteus maximus muscle causes external rotation of the left femur, as well as extension of the left femur in the left hip joint, is the "fact" that the gluteus maximus muscle's point of insertion on the back of the left upper femur is on the outer (lateral) side of the center of the back of the left femur. The degree of external rotation of the left femur varies considerably in different professional golfers, and I will discuss the biomechanical factors that affect the magnitude of this biomechanical phenomenon in greater detail later in this review paper.
More information on the biomechanics of the downswing's pelvic motion -
presented in a Q&A format
Question number 1:
Can you offer swing tips (swing thoughts) that can usefully promote the acquisition of a pro golfer's type of rotary pelvic motion (rather than a hip spinning type of rotary pelvic motion) in a student golfer, and can you describe which swing thoughts are potentially harmful because they can predispose to excessive hip spinning or too much left-lateral shift of the pelvis?
Answer:
I realise that providing a significant amount of background information on golf swing biomechanics is not necessarily helpful to golfers who are not deeply analytical, and I realise that they would prefer more practical swing tips (swing thoughts). So, here is some practical advice that may help a student golfer perform a pro golfer's type of rotary pelvic motion - rather than a hip spinning type of rotary pelvic motion.
I think that a student golfer needs to adopt two swing thoughts at the start of his downswing if wants to learn how to efficiently perform a pro golfer's type of rotary pelvic motion during phase 1 of the "left hip clearing" action - i) maintain, or even momentarily increase, a high degree of weight-pressure loading of the right leg/foot so that the right leg can be "stabilised" - while the isotonic contraction of the right-sided lateral pelvic rotator muscles (that happens subconsciously) causes the pelvis to rotate counterclockwise away from the "stabilised" right leg/foot; and ii) perform the "left hip clearing" action as described by Ben Hogan in his golf instructional book [2] where one basically rotates the left buttocks back towards the tush line in a counterclockwise rotary manner.
Consider the famous diagram from Ben Hogan's book [2].
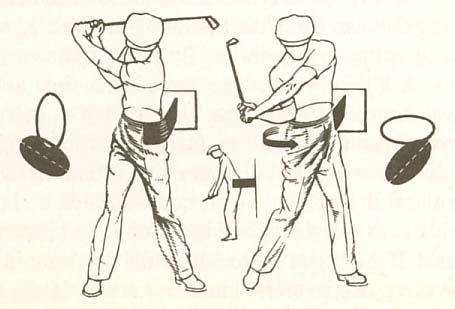
In that diagram, Ben Hogan has a stretched elastic band drawn between the front
of his left pelvis and a wall behind him at his end-backswing position. Then, at
the start of the downswing, he "feels" that the left hip joint area of his left
pelvis is being pulled back towards the tush line in a counterclockwise rotary
manner as the stretched elastic band contracts (shortens). In other words, the
key swing thought for a student-golfer should be the swing thought of "rotating" the left
pelvis back towards the tush line in a counterclockwise rotary manner so that
the pelvis can become square by the end of the early downswing (P5 position).
The simple swing thought of "rotating" the pelvis counterclockwise (as described)
should subconsciously cause a contraction of both the right-sided and left-sided
lateral pelvic rotator muscles, which in tandem should produce the pro golfer's
type of rotary pelvic motion. A student-golfer may think that he needs to
consciously activate the right-sided lateral pelvic contractor
muscles in order to induce a counterclockwise rotation of the pelvis away from a
weight-pressure loaded, and therefore "stabilised", right leg/foot, but I do not
believe that it is necessary. The human brain automatically/naturally knows that
it needs to activate the right-sided lateral pelvic rotator muscles if a
decision is made to rotate the pelvis counterclockwise by "rotating" the left
side of the pelvis back towards the tush line. However, it is
biomechanically necessary that the golfer "stabilise" the right femur/leg and
simultaneously ensure that the right foot is solidly grounded against the
resistance of the ground so that the ground can absorb any clockwise torque of
the right foot. A golfer, who is physically capable of generating a lot of
counterclockwise rotary torque of the pelvis, must ensure that he has
spikes/cleats under his right golf shoe that can prevent slippage of the right
foot if he wants to guarantee that the right foot is adequately "stabilised"
during phase 1 of the "left hip clearing" action.
Under conditions of adequate "stability" of the right leg/foot, the pelvis will
automatically/naturally rotate counterclockwise away from the
"stabilised" right leg/foot when the right-sided lateral pelvic rotator muscles
contract, even though the golfer may actually have the "feeling" that he is
"pulling" the left buttocks back towards the tush line. A golfer may also "feel"
his right ankle invert and "feel" and that he is rolling his right foot inwards,
but that experiental biomechanical phenomenon is secondary to
the counterclockwise motion of the pelvis +/- a small degree of targetwards
motion of the right femoral head and right knee that may happen simultaneously
during this early downswing time period if there is a significant amount of
left-lateral shift of the pelvis happening during phase 1 of the "left hip
clearing" action. It is very important that a student-golfer realise that any
"feeling" of his right foot rolling inwards (if it happens) should be a passive "feeling", and
not an active/deliberate action.
I think that there should be no swing thought relating to the right side (right pelvis or right leg/foot) where one thinks of activating the right side of the pelvis in a "pushing" or "thrusting" manner and/or activating the right knee/foot in an active "pushing-away" motion as this may predispose to hip spinning or too much left-lateral pelvic shift (pelvic sliding). In other words, I think that a student-golfer shouldn't think of actively pushing off the inside of the right foot in a targetwards direction, or think of "kicking-in" the right knee towards the ball, or think of isotonically activating the right gluteus maximus muscle because that may induce the right buttocks to prematurely leave the tush line in a hip spinning manner. I think that the most useful swing thought that pertains to the right leg/foot at the start of the downswing should be the "feeling" of stabilising the right leg/foot by maintaining (or even momentarily increasing) the high degree of weight-presure loading of the right foot +/- experiencing the "feeling" of twisting the right foot clockwise solidly against the resistance of the ground. A student-golfer may never even consciously sense the "feeling" of the right foot being twisted clockwise against the resistance of the ground because it is really a reactive phenomenon, that is secondary to the contraction of the right-sided lateral pelvic rotator muscles (which happens subconsciously). If a student golfer consciously tries to twist the right foot clockwise against the resistance of the ground as an "active action", then he is deliberately trying to create an "active ground reaction force" that may predispose to a right hip spinning type of pelvic rotary motion.
Some golf instructors advise their student-golfers to actively twist their right foot clockwise against the resistance of the ground in order to trigger a counterclockwise rotary pelvic motion.
Consider an example - by Michael Jacobs [3].
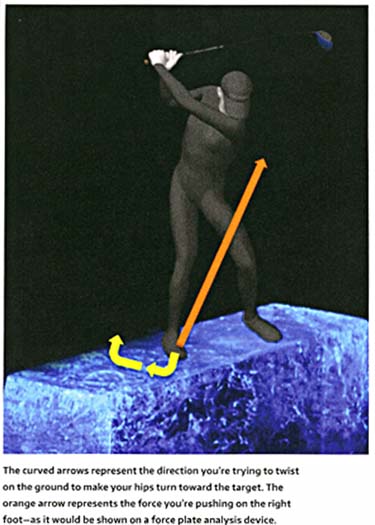
Image copied from reference number [3]
The text in that image states that a golfer must think of twisting the right
foot clockwise against the resistance of the ground (represented by the yellow
arrows) in order to create a ground reaction force that is directed in the
direction of the orange arrow, and Michael Jacobs believes that this ground
reactive force will make the pelvis rotate counterclockwise
around the center-of-rotation (COM) of the body (according to Newtonian
principles of motion). This "belief" comes directly from Dr. Young-Hoo Kwon, who
promotes a *theory that the counterclockwise rotation of the pelvis during the
downswing is due to ground reactive forces acting on the center-of-rotation
(COM) of the body via the Newtonian physical mechanism of a moment force and a
moment arm.
( * I have no sympathy for Dr. Kwon's Newtonian-based theory and I may write a critical review paper comparing his physical-based theory to my biomechanics-based theory, that is based on well-established/sound principles of golf swing biomechanics and kinesiology).
Here is the text from Michael Jacobs' book [3] that accompanies this image-: "Suspend reality for a second and imagine you're standing on a sheet of ice. Without using a ball get in your normal stance. Now, make a slow backswing, and as your body gets close to the end of its turn away from the ball, feel it slow down even more while at the same time push with your right (trailing) foot as though you are trying to spin it away from the target. With your foot flat on the ground and spikes on, it won't actually spin out, but the pressure you are creating will trigger your hips to translate and turn in the opposite direction - toward the target".
Note that Michael Jacobs' bold-highlighted text claims that the pressure that a golfer is creating under the right foot (when he twists his right foot clockwise against the resistance of the ground) will trigger the pelvis to rotate counterclockwise (according to Newtonian principles of motion). I personally believe that he is mixing up "cause-and-effect" because I believe that the true "cause" of the counterclockwise rotation of the pelvis at the start of the downswing in a skilled professional golfer (who executes the pro golfer pattern of pelvic motion) is due to the muscular contraction of the right-sided lateral pelvic rotator muscles, and that any twisting pressure-sensation experienced under the right foot in a clockwise direction during that time period is an "effect" due to the contraction of the right-sided lateral pelvic rotator muscles attempting to externally rotate the right femur/leg against the resistance of the ground while the right leg/foot is being "stabilised" by the golfer actively weight-pressure loading the right leg/foot.
Consider the perspective of another golf instructor - Brian Manzella - who has also been influenced by Dr. Young-Hoo Kwon's ideas on ground reaction forces.
Here is link to a Brian Manzella video lesson (relating to his personal interpretation of Adam Scott's golf swing)
http://www.golf.com/video/learn-adam-scotts-secret-power-move
Here are capture images from his video.

Image 1 shows Brian Manzella at the mid-backswing position. In the video lesson,
he states that a golfer should think of getting his center-of-pressure (COP)
over to his right foot, so that by the time he gets his clubshaft parallel to
the ground he already has 70% of his overall COP-measurement under his right
foot.
Then, Brian Manzella states that a golfer should push upwards in the direction of his right ear to "get force into one's backswing". I think that his assertion that a golfer should push up towards his right ear makes no sense from a biomechanical perspective because it will only predispose to an exaggerated use of an arch-extension maneuver that may predispose to a loss of one's spine bend inclination angle as the right side of the mid-upper body extends or it may even predispose to reverse pivoting (as seen in image 2). Adam Scott obviously doesn't suffer from either a loss of his spine bend inclination angle (or reverse pivoting) in his backswing action. I suspect that Adam Scott is progressively increasing his COP measurement under his right foot from ~50% of his overall COP-measurement at address to 70-80% of his overall COP-measurement by his end-backswing position. By increasingly weight-pressure loading his right leg/foot during his backswing action, he can prevent any swaying motion of his right leg/pelvis away from the target during his backswing action. I also don't think that Adam Scott is actually pushing upwards from his right foot in the direction of his right ear (as Brian Manzella claims) and I think that he is basically pushing his right foot downwards into the ground as he progressively weight-pressure loads his right leg during his backswing action, and that will allow him to efficiently "stabilise" his right leg during both his backswing action and also at the critical transitional moment when he transitions to the start of his downswing action.
To start the downswing, Brian Manzella states that a golfer should push off the right foot in order to move the ground force vector (which was previously directed towards the right ear) to a direction that is left of the left ear so that the changing ground force vector can cause the lower body to rotate around the body's center-of-rotation (COM) and he states that when the left arm is parallel to the ground (image 3) that a golfer should have 70% of his overall COP-measurement already under his left foot. Then, he states that from the P5 position (image 3) to impact, that a golfer should only push upwards towards his left ear, which will secondarily cause a straightening of his left leg (as seen in image 4).
In other words, Brian Manzella thinks that the changing ground reaction forces generated under the two feet are causing Adam Scott's rotary pelvic motion during his downswing and that it is also causing the straightening of his left leg as he pushes upwards towards his left ear from his weight-pressure loaded left foot in his later downswing. I totally disagree with his explanation, and I think that Brian Manzella is simply imposing his Dr. Kwon-derived explanatory theory on Adam Scott's swing. I think that my biomechanical explanation better explains Adam Scott's downswing action. I think that Adam Scott starts his downswing's rotary pelvic motion by activating his right-sided lateral pelvic rotator muscles (while weight-pressure loading his right leg/foot, which will "stabilise" his right femur so that his pelvis can rotate counterclockwise away from his "stabilised" right leg) and that biomechanical muscular action will get his pelvis square by the P5 position, where he will likely have 50% of his overall COP-measurement under each foot. Adam Scott will then straighten his left leg in his later downswing secondary to the activation of his left knee extensor muscles and that will cause elevation of his left pelvis as the left hip joint moves further away from his solidly grounded left foot (which probably has 70-80% of his overall COP-measurement located under his left foot at impact because Adam Scott manifests the swing biomechanics of a * "front foot" golfer).
(* I will explain the different swing biomechanics between a "front foot" golfer and a "reverse foot" golfer later in this review paper)
I don't think that Adam Scott is actively pushing off his right foot at the start of his downswing to any significant degree in either a targetwards direction (that can predispose to excessive pelvic sliding) or in a direction that is more outwards towards the ball that can predispose to hip spinning.
Here are capture images from a DTL video of Adam Scott's driver swing.

Imag 1 shows Adam Scott at his end-backswing position. I have drawn a red line
against the back of his right buttocks and that represents his tush line.
Image 2 shows Adam Scott at the P4.5 position. Note that he is rotating his left buttocks back towards the tush line in a hip-squaring manner (as described by Ben Hogan in his "left hip clearing" action diagram) while still keeping his right buttocks back against the tush line.
Image 3 shows Adam Scott at the P5 position with a square pelvis. Note that his right buttocks is still against the tush line, which means that he is not a right hip spinner.
Image 4 shows Adam Scott at the P5.5 position. Note that his right buttocks is now leaving the tush line and that his pelvis is slightly open. However, note that he can get easily his right elbow well in front of his right hip area by P5.5 and that his right elbow is not being "blocked" by his right pelvis. Note that his right heel is not elevated off the ground and note that his right knee is not "kicked-in".
Now consider Rory McIlroy's pelvic motion during the early-mid downswing.
Here are capture images from a DTL swing video of Rory McIlroy's driver swing.

Image 1 shows Rory McIlroy at his end-backswing position. I have drawn a red
line against the back of his right buttocks and that represents his tush line.
Image 2 shows Rory McIlroy at the P4.5 position. Note that he is rotating his left buttocks back towards the tush line in a hip-squaring manner (as described by Ben Hogan in his "left hip clearing" action diagram) while still keeping his right buttocks back against the tush line. Note that Rory McIlroy manifests far more knee and hip joint flexion than Adam Scott at the start of his downswing.
Image 3 is at the P5 position. Note that Rory McIlroy has got his pelvis more than slightly square and note that his right buttocks is already starting to leave the tush line, which indicates that he has an element of a right hip spinning action.
Image 4 is at the P5.5 position. Note that Rory McIlroy's pelvis is more open than Adam Scott's pelvis at his P5.5 position. Note that his right buttocks is well forward of his tush line, and that he has elevated his right heel and kicked-in his right knee towards the ball - and those biomechanical features are suggestive of a small degree of right hip spinning. Note that the forward-and-outward motion of his right pelvis (due to an element of right hip spinning) gives him less room in front of his right hip area to position his right elbow, and that his right elbow is therefore positioned more alongside his right hip area. That biomechanical phenomenon where the right pelvis is potentially "blocking" the right elbow's path is a well known side-effect of a right hip spinning motion. Rory McIlroy usually doesn't have a "blocking" problem when he is swinging rhythmically and ultra-smoothly, but occasionally he has too much right hip spinning motion that produces "blocking" and resultant wayward drives.
Many professional golfers occasionally complain of being "blocked" during their mid-downswing, and Tiger Woods has frequently stated that it is has been a lifelong problem that he has had to deal with throughout his professional career.
Here is a link to a you-tube video (dating from the early 2000s) where Tiger Woods (together with his coach Butch Harmon) discuss this "blocking" problem
https://www.youtube.com/watch?v=xOecUNBV_Q0
Between the 2.00-2:33 minute time point of the video, Tiger Woods describes his "ole swing" where he got "stuck" because his right hip was blocking his right elbow at the P5.5 position.
Here is a capture image from the video.
In that capture image, note that Tiger Woods is demonstrating being "stuck",
which is causally due to an over-assertive right hip spinning motion that
"blocks" his right elbow.
In the video, Tiger Woods describes a Butch Harmon-inspired drill where he had to endlessly practice "getting his arms/club more in front of him". I believe that Butch Harmon's advice/drill represented a band-aid approach that didn't really work well over the long term because Tiger Woods continued to suffer from the same "blocking" problem in his later career. I think that it would have been better if Tiger Woods dealt with the "true" causal issue - a right hip spinning problem - and the optimum solution may have been a change in the pattern of his rotary pelvic motion to a pro golfer's type of rotary pelvic motion (as prototypically manifested by Adam Scott).
Although right hip spinning may occasionally cause a "blocking" problem in skilled professional golfers, it can become a much greater problem in unskilled amateur golfers who start their downswing's pelvic motion by "kicking-in" their right knee while simultaneously activating their right gluteus maximus muscle. That biomechanical combination can produce an exaggerated degree of right hip spinning that causes them to spin around their left leg while falling backwards onto their right foot. An exaggerated degree of right hip spinning can also predispose to roundhousing of the upper body if the unskilled golfer rotates his upper torso in unison with his pelvis, and that biomechanical combination can cause an OTT move and out-to-in clubhead swingpath through impact.
Now, let's consider the topic of pelvic shift, and consider whether any left-lateral pelvic shift towards the target must precede a counterclockwise rotary motion of the pelvis during the early downswing.
Many golf instructors believe that a golfer must start the downswing with a left-lateral shift of the pelvis towards the target before they start to rotate their pelvis counterclockwise, but I believe that their recommended "shift-then-rotate" pelvic motional swing pattern can produce a suboptimal pelvic motion during the downswing.
Consider some examples of that type of golf instructional teaching.
Example number 1 - Mark Panigoni swing video lesson - https://www.youtube.com/watch?v=4eVd0xjIR1I
Here is a capture image from the 1:50 minute time point of the video where Mark Panigoni demonstrates how one should slide the pelvis targetwards before one rotates the pelvis.

The above image shows Mark Panigoni at the P5.5 position.
I have drawn a red arrowed line vertically down from the outer border of his left
pelvis and it strikes the ground outside the outer boundary of
his left foot.
I believe that the outer border of the left pelvis should never get outside the left foot at any time during the downswing time period, and I believe that it will likely predispose to pushed shots (if the hands get too far ahead of the clubhead by impact - especially if it is associated with an incomplete release of PA#3).
Consider another example.
Example number 2 - Andrew Rice video lesson - https://www.youtube.com/watch?v=ixPSMG1m9Sc
In that drill, Andrew Rice positions the outer border of his left foot/pelvis about 4" from the wall, and he then states that one should drive the left side of the pelvis into the wall.
Here are capture images from that video showing Andrew Rice demonstrating that drill (without a golf club).

Image 1 shows Andrew Rice at address. Note that the outer border of his
left pelvis is about 4-6" away from the wall.
Image 2 shows Andrew Rice at the P5.5 position - with the left side of his pelvis pressed against the wall.
I think that this is a terrible golf instructional drill that will teach a student golfer a sub-optimal type of "shift-then-rotate" type of pelvic motion pattern.
Consider another example.
Example number 3 - Sean Foley video lesson - https://www.youtube.com/watch?v=JHuyVf7ulKE
Here are capture images from that Sean Foley video.

Sean Foley has positioned two red poles just outside the outer border of both
his left foot and his right foot. Note that he has folded his two arms across
the front of his chest because he only wants to demonstrate his desired pivot
motion.
Image 1 shows Sean Foley at address. Note that his pelvis is roughly centered between his feet.
Image 2 shows Sean Foley at his end-backswing position. Note that the distance between the outer border of his right pelvis and the red pole (alongside his right foot) has increased because Sean Foley has "turned inside" his right hip during his backswing's rotary pelvic action. I agree with Sean Foley that one shouldn't "turn-over" the right hip using a swaying motion of the right thigh combined with a rightwards-leaning motion of the upper body (which he demonstrates in his video) and I agree with Sean Foley that his "turning inside" his right hip is the optimal pelvic motional technique - where the pelvis remains roughly centered between the feet and where there is no weight shift (COM-shift) during the backswing action.
Image 3 shows how Sean Foley recommends that a golfer start the pelvic motion during the downswing - by shifting the lower swing center (shifting the lower COM of the body) towards the target. Note how the left side of his pelvis and left upper thigh are crashing against the red pole that is positioned just outside his left foot.
I believe that Sean Foley's variation of a "shift-then-rotate" pelvic motional pattern is suboptimal, and I think that a student-golfer should never think of shifting his body weight (COM) leftwards during the downswing action if he wants to perform the pro golfer's pattern of rotary pelvic motion.
Consider this golf instructional video that was filmed in 1953 (long before the era of force plate technology and the era of COP-measurements)
https://www.youtube.com/watch?v=yHvCzmi8FzU
It's an interesting video that is worth watching - if only to see the swings of famous golfers like Sam Snead, Ben Hogan and Lew Worsham.
Here is a link to a shorter (unedited) version of that video that shows the golf instructor teaching a "no-weight shift" type of pivot motion.
https://www.youtube.com/watch?v=Hk33ksSHFvc
That golf instructor uses Lew Worsham as an example of how a golfer should only think of performing a centered rotary pivot motion during the downswing - without ever thinking of deliberately shifting any body weight (COM) from right-to-left in a targetwards direction. He states that any small degree of weight shift that may happen during the downswing will happen naturally during the rotary pivot motion. I think that it is highly likely that there is very little body weight shift (COM-shift) happening during Lew Worsham's downswing action - although there is likely to be a significant shift of his overall COP-measurement from right-to-left during his downswing action. Lew Worsham likely has 70-80% of his overall COP measurement under his right foot at his end-backswing position and then 70-80% of his overall COP-measurement under his left foot at impact. That represents a large shift from right => left in terms of COP-measurements (which are a measure of weight-pressure loading and not a measure of COM-shift), and there is no apparent targetwards shift of his torso during his downswing action. His torso remains remains roughly centered between his feet during his entire downswing action.
Here are birds-eye view capture images of Lew Worsham's early downswing action (from that video).

Image 1 shows Lew Worsham at his end-backswing position (P4 position). I have
drawn a red line against the outer border of his right pelvis and a blue line
against the right side of his left lower thigh.
Image 2 and 3 show his early downswing's rotary pelvic motion. Note how he squares his pelvis by P5 (image 3) by contracting his right-sided lateral pelvic rotator muscles (that rotate his pelvis counterclockwise away from his "stabilised" right leg) - and note that there is very little left-lateral pelvic shift motion of his pelvis away from that red line during his rotary pelvic motion. His pelvis only shifts a few inches left-laterally and it happens while he is rotating his pelvis counterclockwise. Note that his left thigh is being abducted and externally rotated away from that blue line due to the muscular contraction of his left-sided lateral pelvic rotator muscles (in combination with the "fact" that his pelvis, and therefore left hip joint, is rotating counterclockwise back towards the tush line as a result of the contraction of the right-sided lateral pelvic rotator muscles). Note how his body remains roughly centered between his feet during his downswing's rotary pelvic motion.
Now, consider birds-eye view capture images of Arnold Palmer's and Jack Nicklaus' downswing from this swing video
https://www.youtube.com/watch?v=StKkT9sTTtQ
Arnold Palmer's downswing action
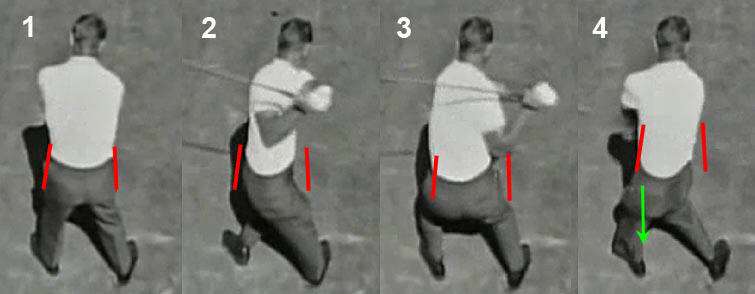
Image 1 shows Arnold Palmer at address. I have drawn red lines alongside the
outer border of his left pelvis and right pelvis. Note that his pelvis is nearly
centered between his feet at address, and it is only slightly closer to
his left foot.
Image 2 shows Arnold Palmer at his end-backswing position. Note that Arnold Palmer rotates his pelvis about 60-70 degrees clockwise during his backswing action, but it rotates clockwise without any swaying motion of his pelvis or his upper torso. Note that there is apparently no body weight shift (COM-shift) during his backswing's centered pivot motion. Arnold Palmer is basically "turning into" his right hip joint, and his right femoral head becomes internally rotated in his right hip joint at his P4 position because he rotates his pelvis clockwise much more than he rotates his right femur clockwise.
Image 3 shows Arnold Palmer at the P5 position (end of the hip-squaring phase). Note that he squares his pelvis by rotating his pelvis counterclockwise by ~60-70 degrees during the P4 => P5 time period. Note that he rotates his left buttocks back towards the tush line, without allowing his right buttocks to prematurely leave the tush line in a right hip spinning manner. Note that the outer border of his left pelvis never shifts left of that left-red line, which means that there is no preliminary left-lateral pelvic shift happening during his early downswing's rotary pelvic motion.
Image 4 shows Arnold Palmer at impact. I have drawn a green-arrowed line vertically downwards from the outer border of his left pelvis - note that it shows that the outer border of his left pelvis is still inside his left foot at impact and that it is vertically aligned with that left-red line.
Jack Nicklaus' downswing action

Image 1 shows Jack Nicklaus at address. I have drawn red lines alongside the
outer border of his left pelvis and right pelvis. Note that his pelvis is
centered between his feet.
Image 2 shows Jack Nicklaus at his end-backswing position. Note that he has rotated his pelvis about 60 degrees clockwise during his backswing by "turning into" his right hip. Note that his right femur is internally rotated in his right hip joint because he rotated his pelvis clockwise more than he rotated his right femur. Note that he manifested a centered pivot motion during his backswing action and that there is likely no COM-shift happening during his backswing action.
Image 3 is at the P5 position (end of the hip-squaring phase). Note that Jack Nicklaus basically rotated his left buttocks back towards the tush line while still keeping his right buttocks against the tush line. Note that the outer border of his left pelvis has only moved a few inches left of the left-red line, and that small degree of left-lateral shift of his pelvis happened while he was rotating his pelvis counterclockwise.
Image 4 shows Jack Nicklaus at impact. I have drawn a green-arrowed line vertically downwards from the outer border of his left pelvis - note that it shows that the outer border of his left pelvis is still inside his left foot at impact and that it is nearly vertically aligned with that left-red line.
Both Arnold Palmer and Jack Nicklaus exhibit a very centered pivot motion during both their backswing and downswing, and there is likely very little COM-shift happening during their centered pivot motion. Both golfers also do not manifest a "shift-then-rotate" type of pelvic motion, and they simply rotate their torso between their feet with very little left-lateral pelvic shift happening during their downswing's counterclockwise pelvic rotational motion.
Now, let's consider some factors that will often determine the amount of left-lateral pelvic shift that will naturally happen during the downswing of a professional golfer if he uses a pro golfer's pattern of pelvic rotary motion.
Consider David Leadbetter's artist-drawn image of a golfer "rotating in a barrel" (copied from David Leadbetter's book "The Golf Swing").
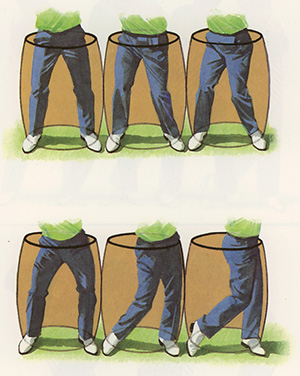
The composite image shows a golfer "rotating-in-a-barrel" as he performs a full
golf swing action. Note that the width of the barrel's opening is determined by
the width of the golfer's stance and it is wider than the width of the pelvis -
and a wider stance width is a common golf swing choice when a golfer uses a
driver, rather than a short-iron.
Note that the golfer's pelvis is centered in the barrel opening at address (see top-left image). Note that the golfer used a centered pelvic loading motion technique during his backswing action - where the pelvis remains centered in the barrel opening at the end-backswing position (see top-right image). The bottom-left image shows the golfer at the end of his hip-squaring phase (where he manifests the Sam Snead "sit-down" look) - note that his pelvis is still nearly centered in the barrel opening. The bottom-center image shows the golfer at impact - note that the outer-left border of his pelvis is positioned against the left side of the barrel opening, which means that the golfer shifted his pelvis left-laterally during phase 2 of the "left hip-clearing action" and he has allowed the outer border of his left knee to move outside the outer border of his left foot. Note that his straightened left leg is near-vertical at impact, and that is a characteristic biomechanical feature of a "front-foot" golfer.
Note that Jack Nicklaus fits into this particular variant of a "rotating-in-a-barrel" pattern - because his left knee moves outside the outer border of his left foot as the left side of his pelvis abuts against the left side of the barrel opening during his later downswing.

Image 1 shows Jack Nickaus at address with his pelvis centered in the barrel
opening.
Image 2 shows Jack Nicklaus at his end-backswing position with his pelvis slightly left-of-center within the barrel opening.
Image 3 shows Jack Nicklaus at the end of his hip-squaring phase - note that his pelvis is getting closer to the left side of the barrel opening.
Image 4 shows Jack Nicklaus at impact. Note that the left side of his pelvis is nearly abutting against the left side of the barrel opening, while the outer border of his left knee is outside the outer border of his left foot.
Jack Nicklaus was known to incorporate a certain amount of targetwards "drive of his knees" during his downswing action, which partly accounts for the left-lateral shift of his pelvis during his downswing's rotary pelvic motion.
Now consider, how this "rotating-in-a-barrel" imagery applies to Jamie Sadlowski's downswing action.

Note that I have drawn a yellow-colored, elliptical-shaped image over the Jamie
Sadloski capture images, and that will represent the opening of a barrel that
has an opening width equal to the width of his stance.
Image 1 shows Jamie Sadlowski at his end-backswing position. Note that his pelvis is centered in the barrel opening because he used a center-loading pelvic motion technique during his backswing action.
Image 2 shows Jamie Sadlowksi at the end of his hip-squaring phase and there has been very little left-lateral shift of his pelvis towards the target.
Image 4 shows Jamie Sadlowski at impact. Note that his pelvis has shifted a very small amount left-laterally, but the outer-left border of his pelvis never reaches the left side of the barrel opening because his left leg is slanted well away from the target, and that is a characteristic biomechanical feature of a "reverse-foot" golfer.
Now consider the pelvic motion pattern of Mickey Wright, who is regarded by many golf commentators as the greatest female golfer in the history of golf - winning 86 LPGA golf tournaments. Ben Hogan even stated that he thought that she had the "finest swing that he had ever seen"!
Consider a swing video of her driver swing action - https://www.youtube.com/watch?v=JQhWRshs6Zs
Here are capture images from her swing video.

Note that I have drawn a yellow-colored, elliptical-shaped image over Mickey
Wright's capture images, and that will represent the opening of a barrel that
has an opening width equal to the width of her stance.
Image 1 shows Mickey Wright at her end-backswing position. Note that she used a right-loading pelvic motion technique during her backswing action that gets her pelvis much closer to the right side of the barrel opening at her end-backswing position. I have also drawn a red line against the right side of her pelvis at her end-backswing position (as a reference point).
Image 3 shows Mickey Wright at the end of her hip-squaring phase, where she manifests the Sam Snead "sit-down" look. Note that her pelvis is centered in the barrel opening, which means that she shifted her pelvis a few inches left-laterally during her hip-squaring phase, and that biomechanical phenomenon happens naturally while she rotates her pelvis counterclockwise (secondary to the contraction of her right-sided and left-sided lateral pelvic rotator muscles).
Image 5 shows Mickey Wright at impact. Note that her pelvis only moves left-laterally by a very small amount during phase 2 of her "left-hip clearing" action, and she never allows the outer-left border of her pelvis to reach the left side of the barrel opening at impact (as seen in David Leadbetter's golfer-image) even though she is likely a "front foot" golfer, who likely has ~80% of her overall COP-measurement located under her left foot at impact. Note that the outer border of her left knee is not outside the outer border of her left foot. She doesn't "drive her knees" towards the target during her later downswing (like Jack Nicklaus) and she is efficiently bracing her left leg (which is becoming more weight-pressure loaded) to prevent any left-lateral pelvic slide motion during phase 2 of her "left hip clearing" action.
These three examples demonstrate that three factors (in variable degrees of combination) can naturally cause a variable amount of left-lateral pelvic shift during the skillful execution of a pro-golfer's pattern of rotary pelvic motion during the downswing - i) a stance width that is wider than the width of the pelvis, ii) a right-loading pelvic motional technique during the backswing action and iii) any tendency to shift the pelvis left-laterally during phase 2 of the "left hip clearing" action so that the outer border of the left knee gets outside the outer border of the left foot by impact.
In those three examples of Jack Nicklaus, Jamie Sadlowski and Mickey Wright hitting a driver, the three golfers are using a "rotating-in-a-barrel" swing style where the pelvis remains within the inner boundaries of the barrel opening during their entire downswing action. That phenomenon doesn't usually happen when professional golfers hit short irons shots using a very narrow stance where their stance width is roughly equal to their pelvis width. Under those circumstances, professional golfers often allow their pelvis to sway left-laterally so that their lower swing center moves targetwards by many inches, and the outer border of their left pelvis gets well outside the outer boundary of their left foot by impact. That "pelvic shift" type of pelvic motional technique is a very different pelvic motional technique than a pro golfer's rotary pelvic motional technique (where the golfer is "rotating-in-a-barrel" with a variable amount of pelvic shift), and it allows them to come down steeper onto the ball, so that they can generate a steeper clubhead attack angle.
Question number 2:
You stated that the right-sided lateral pelvic rotator muscles are primarily responsible for rotating the pelvis between P4 and P5, and that the left-sided gluteus maximus muscle plays an important role in the later downswing between P5 and impact. What is the potential role of the right gluteus maximus muscle in generating pelvic rotary motional power during the downswing?
Answer:
Theoretically, it would seem that the right gluteus maximus muscle could play a significant role in rotating the pelvis counterclockwise during the downswing (especially in golfers who use a right hip spinning pattern of rotary pelvic motion), but if the right gluteus maximus muscle isotonically contracted to a significant degree at the very start of the early downswing, then it would cause early extension (and posterior pelvic tilt) because it is primarily a hip extensor muscle. As I have already described in my biomechanical description of a pro golfer's pattern of rotary pelvic motion - most professional golfers, who use that pattern of rotary pelvic motion during phase 1 of their "left hip clearing" action, either maintain their degree of spine bend inclination (and therefore their degree of anterior pelvic tilt) between P4 and P5, or they momentarily increase their degree of hip joint flexion (and thereby momentarily increase their degree of spine bend inclination angle and anterior pelvic tilt) between P4 and P5. However, that "fact" doesn't mean that their right gluteus maximus muscle is not isometrically active during the P4 => P5 time period. Their right gluteus maximus muscle could be isometrically active between P4 and P5, and it could then become isotonically active between P5 and impact.
Consider Jamie Sadlowski's pelvic motion during his downswing action.
Jamie Sadlowski swing video - https://www.youtube.com/watch?v=DB-L9wkNO6c
Here are capture images from that swing video.

Image 1 shows Jamie Sadlowski at his end-backswing position. I have drawn a red
line against the back of his right buttocks and that represents the tush line.
Image 2 shows Jamie Sadlowski's early downswing pelvic motion - note that he is rotating his left buttocks back towards the tush line while still keeping his right buttocks close to the tush line.
Image 3 shows Jamie Sadlowski at the end of his hip-squaring phase (phase 1 of his "left hip clearing action"). Note that his pelvis is square and that he rotated his left pelvis counterclockwise during his early downswing so that his left buttocks nearly reaches the tush line - while still keeping his right buttocks close to the tush line. Note that he acquired an increased degree of hip joint flexion (and therefore more anterior pelvic tilt) during his early downswing due to an isotonic contraction of his iliopsoas muscle. During this time period, his right gluteus maximus muscle could be isometrically active to a significant degree.
Image 4 shows Jamie Sadlowski at the P5.5 position. Note how his right buttocks has moved outwards away from the tush line, and note that his right hip joint is far less flexed. That biomechanical combination suggests that Jamie Sadlowski could be isotonically contracting his right gluteus maximus muscle, which implies that it could then be contributing to his rotary pelvic motion between P5 and impact (during phase 2 of his "left hip clearing" action).
I previously mentioned that if the right gluteus maximus muscle was over-active during the early downswing that it could predispose to a premature outward motion of the right buttocks away from the tush line, which could then result in a right hip spinning phenomenon and therefore a "blocking" problem when the golfer reaches the P5.5 position. Theoretically, a "blocking" problem could still occur if a golfer delayed the isotonic contraction of his right gluteus maximus muscle so that any right hip spinning phenomenon only happens between P5 and P5.5 (and not between P4 and P5) - if the degree of outwards motion of the right pelvis is excessive. However, I think that a "blocking" problem is unlikely to happen in long-drive competitors because they do not usually get their right elbow down to a low position that is directly in front of their right hip area at the P5.5-P6 position. Most long-drive competitors swing their clubshaft down the turned shoulder plane (TSP) during their entire downswing and they do not shallow their clubshaft down to the elbow plane (or even lower to the hand plane - like Ben Hogan) during their mid-late downswing.
Consider Jamie Sadlowski's clubshaft motion during his downswing action.
Jamie Sadlowski DTL swing video - https://www.youtube.com/watch?v=ci97GM-hxbk
Here are capture images from the swing video.
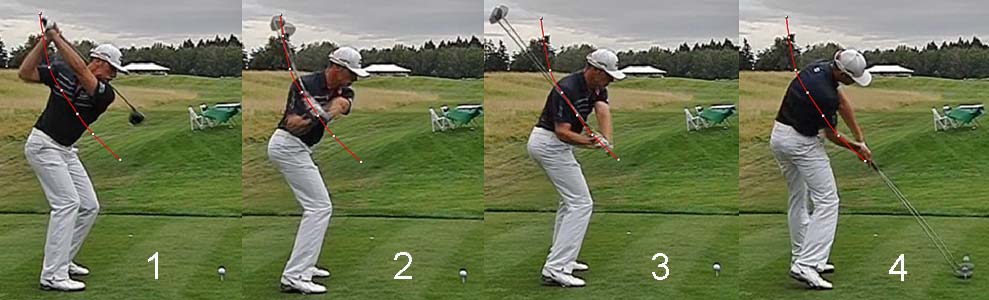
Image 1 shows Jamie Sadlowski at his end-backswing position. Note that his hands
are positioned only slightly higher than the turned shoulder plane (TSP).
The red splined path represents his hand arc path during his downswing action - note that his hand arc path crosses his right shoulder and comes down the TSP in the direction of the ball.
Image 2 shows Jamie Sadlowski at the P5 position. Note that his hands and clubshaft have descended down the TSP without any clubshaft shallowing.
Image 3 shows Jamie Sadlowski at the P5.5 position. Note that his hands and clubshaft are still descending down the TSP. Note that his right elbow is well above his right hip area, which means that it cannot easily become "blocked" by any excessive right hip spinning motion.
Image 4 shows Jamie Sadlowski at impact. Note that his clubshaft and hands are still on the TSP and there has been no planar shift of his clubshaft during his entire downswing action. Note that his left arm is outstretched away from his body and that his right elbow is far away from his right pelvis.
In other words, if a long-drive competitor's hands/clubshaft comes down the TSP and if he does not shallow his clubshaft during his downswing action, then he will not seemingly have a significant risk of experiencing a "blocking" problem - even if his right pelvis spins outwards too much during his early-mid downswing action. That "fact" means that a long-drive competitor can isotonically activate his right gluteus maximus muscle in an attempt to maximise his speed of pelvic rotation. However, that "fact" may not apply to a PGA tour golfer, or a skilled amateur golfer, who shallows his clubshaft to the elbow plane (or hand plane) during his mid-downswing, because a right hip spinning phenomenon (due to an isotonic contraction of his right gluteus maximus muscle) may predispose him to a significant risk of experiencing a "blocking" problem. Caution should be exercised by a golfer, who is thinking about the possibility of increasing the speed of his pelvic rotary motion via the isotonic contraction of his right gluteus maximus muscle, because the potential disadvantages related to that choice may exceed the potential advantages.
Question number 3:
Why does Rory McIlroy's pelvic rotary motion seem to stall at the P6 position?
Answer:
Consider Rory McIlroy's driver swing - https://www.youtube.com/watch?v=H4_BRVrUOHU#t=44
Here are capture images from the swing video.

Image 1 is at the end-backswing position. I have drawn a blue line at the top of
his head to mark his head position.
Image 2 is the start of his downswing's pelvic rotary motion and image 3 is at the end of his hip-squaring phase (phase 1 of the "left hip clearing" action). Note that he has the Sam Snead "sit-down" look with dual-ER of both thighs in their respective hip joints at the end of his hip-squaring phase. Note that his head has dropped a few inches due to the increased degree of hip and knee flexion that is happening during his hip-squaring phase. The counterclockwise rotation of his pelvis during phase 1 of the "left hip clearing" action is primarily due to the contraction of his right-sided lateral pelvic rotator muscles and secondarily due to an isometric contraction of his left adductor magnus muscle. Note that his left knee doesn't move targetwards very much between P4 and P5 because his left femur was not internally rotated and adducted at the P4 position.
Image 4 is at the P6 position. Note that his pelvis is open relative to the ball-target line, that his right knee is "kicked-in", that his right heel is raised, and that his right hip joint is less flexed - and those biomechanical features suggest that he is isotonically contracting his right gluteus maximus muscle. Note that his left hip joint is in a state of internal rotation because he has rotated his pelvis more counterclockwise than his left femur between P5 and P6. His left adductor magnus muscle is isonically contracting during this time period, which will pull his left inferior pubic ramus closer to his left femur - thereby contributing to the counterclockwise rotation of his pelvis between P5 and P6.
Image 5 is at impact and image 6 is at the P8 position. Note that his pelvis has not rotated more counterclockwise between P6 and P8, even though he has straightened his left leg and elevated his left pelvis due to the isotonic contraction of his left knee extensor muscles and left gluteus maximus muscle. His straightened/braced left leg is likely associated with increased weight-pressure loading of his left foot, and this "biomechanical combination" impedes any further rotation of his pelvis in a counterclockwise direction - and it is important to realise that this "biomechanical combination" is happening when the muscles (right-sided lateral pelvic rotator muscles, right gluteus maximus muscle and the left adductor magnus muscle) that have rotated his pelvis counterclockwise between P4 and P6 are already fully contracted, so it is not surprising that his pelvis doesn't rotate counterclockwise any more between P6 and P8. Most professional golfers similarly exhibit a distinct slowing of their speed of rotary pelvic motion between P6 and impact - for the same biomechanical reasons.
Question number 4:
Should a golfer lift the left heel during the backswing action and is it associated with increased swing power. Secondly, should a golfer then first replant the left heel on the ground by shifting his body weight targetwards before he starts his downswing's counterclockwise rotary pelvic motion (representing phase 1 of the "left hip clearing" action where the left buttocks gets rotated back towards the tush line)?
Answer:
If you look at professional golfers in the 1930-1950 era, many of them manifested a large degree of clockwise rotation of their pelvis during their backswing action and they often lifted their left heel well off the ground as they adducted their left knee towards their right knee.
Consider some of these golfers at their end-backswing
position.

Note that all four of these famous golfers from that bygone era manifested a
large degree of clockwise rotation of their pelvis during their backswing
action, and they all elevated their left heel, which enabled them to more easily
adduct their left thigh so that they could get their left knee very close to
their right knee by their end-backswing position.
Now, consider four superb modern-day golfers.

Note that all four of these famous, modern-day golfers manifest far less
clockwise rotation of their pelvis during their backswing action. Note that they
also keep their left heel planted and they do not elevate their left heel, which
means that they do not adduct their left thigh during their backswing so that
their left knee gets very close to their right knee by their end-backswing
position.
Which is the better choice for a serious student-golfer who wants to learn to play at the highest professional level? Brandel Chamblee (famous Golf Channel TV commentator) obviously prefers the swing action of those famous golfers from a bygone era, and he has written a book [4] on the subject where he states that he has a clear preference for their type of backswing action. However, I know of no biomechanical or scientific reason to support that personal preference, and I believe that it is optional as to whether one should rotate the pelvis clockwise by a greater amount during the backswing + elevate the left heel (like Bobby Jones, Sam Snead, Jack Nicklaus and Arnold Palmer) or whether one should rotate the pelvis far less clockwise during the backswing + keep the left heel planted (like Jason Day, Jordan Spieth, Rory McIlroy and Adam Scott). All four of these modern-day golfers can generate prodigious amounts of swing power, and they definitely can compete in terms of swing power to those four bygone era golfers. How is that possible considering that they have a far smaller range of rotary pelvic motion during their backswing action, and therefore their downswing action?
When I came to appreciate the importance of the right-sided lateral pelvic rotator muscles in generating a counterclockwise rotation of the pelvis between P4 and P5, I also came to appreciate the practical advantages of limiting the amount of clockwise pelvic rotation happening during the backswing (as exemplified by the swings of Jason Day, Jordan Spieth, Rory McIlroy and Adam Scott). Note that all four of these golfers do not allow their right thigh to rotate very much clockwise during their backswing, and that allows them to "turn into their right hip" and establish a state of internal rotation of their right femoral head in their right hip socket (which optimally stretches the right-sided lateral pelvic rotator muscles) without having to rotate their pelvic very much clockwise (compared to those four golfers from a bygone era, who allowed their right thigh to externally rotate much more during their backswing action). If the right hip joint is not rotated clockwise as much during the backswing action, that means that the right femoral head is not moving very far away from the right foot and that allows the right femur to be more vertical, and therefore less angulated, at P4. Under those conditions, it may be biomechanically much easier to more efficiently weight-pressure load ("stabilise") the right leg/foot at the start of the transition to the downswing, and a more efficient "stabilisation" phenomenon will allow the subsequent muscular contraction of the right-sided lateral pelvic rotator muscles to rotate the pelvis counterclockwise with the maximum amount of "rotary torque force". It is amazing to note the magnitude of the rotational angular velocity of the pelvis that Rory Mc Ilroy and Jason Day are capable of generating between P4 and P5 - even though they only rotated their pelvis clockwise by ~40 degrees during their backswing action! I am therefore not surprised to note that many modern-day professional golfers also prefer to limit the amount of clockwise rotation of their pelvis during their backswing - like Rory McIlroy and Jason Day - and the primary reason has nothing to do with the "idea" of generating a large X factor (large degree of torso-pelvic separation) during their backswing action. The primary reason is that it allows them to optimise their loading (stretching) and subsequent unloading (contraction) of their right-sided lateral pelvic rotator muscles, so that they can more efficiently rotate their pelvis counterclockwise (away from their efficiently "stabilised" right leg/foot) with the maximum degree of rotary torque.
Although I can now better understand why so many modern-day golfers prefer to limit their pelvic rotation during their backswing action and keep their left heel grounded, I still think that a student-golfer should remain open-minded about this issue. He can personally experiment by trying both techniques (which are both biomechanically sound) and choose the technique that works best for him.
The second question is whether a golfer, who lifts his heel during his backswing action, has to first replant the left heel on the ground by shifting his body weight targetwards before he starts his downswing's counterclockwise rotary pelvic motion (representing phase 1 of the "left hip clearing" action where the left buttocks gets rotated back towards the tush line)?
Consider this golf instructional video produced by Shawn Clement.
https://www.youtube.com/watch?v=0CSHqnYNijw
Note that Shawn Clement shifts his pelvis left-laterally in a distinct "bump-left" manner in his late backswing. He talks of "settling" and replanting the left foot during his "bump-left" maneuver and he believes that it must happen before he starts to rotate his pelvis counterclockwise. Shawn Clement talks about his pivot rotational action "revolving around his left leg" and he seemingly believes that one must shift one's weight over to the left leg before one can rotate one's pelvis around that weighted/braced left leg. In fact, starting at the 2:39 minute time point of his video, he even claims that Jack Nicklaus performed this "bump-left" maneuver and replanted weight on his left heel before he started to rotate his pelvis counterclockwise. However, that claim is obviously not true! I have previously shown that Jack Nicklaus starts to rotate his pelvis counterclockwise at the very start of his downswing and that he doesn't have to first replant weight on his left heel, and/or first shift his pelvis targetwards, before he starts to rotate his pelvis counterclockwise.
Here is further evidence from a swing video of multiple Jack Nicklaus swings - https://www.youtube.com/watch?v=5ocMJecgW2w
Here are capture images from one of those swings.
![]()
These sequential images show the start of Jack Nicklaus' downswing. Note that
his left heel is still elevated off the ground in the first 4 images (and
probably still elevated off the ground in image 5), and yet there is definite
visual evidence that i) he is rotating his pelvis counterclockwise and ii) also
externally rotating his left femur (which causes his left knee to move
targetwards away from his right knee). In fact, from a biomechanical
perspective, it is much easier to externally rotate the left femoral head in the
left hip joint (secondary to a contraction of the left-sided lateral pelvic
rotator muscles) if the left foot is not significantly weight-pressure loaded
and if it is more "free-floating" in space.
Secondly, note that Shawn Clement refers to the term "weight shift" when he performs his "bump-left" maneuver - but that "weight shift" term is not synonomous with the term "weight-pressure loading".
Consider a comparison between Shawn Clement and Kevin
Streelman as they transition into their early downswing.

Image 1 shows Shawn Clement at the end of his "bump-left" maneuver and he
seemingly believes that he has shifted his body weight (COM) leftwards.
Image 2 shows Kevin Streelman at exactly the same "start of the downswing" position and he looks very similar to Shawn Clement in terms of body posture/positioning. The vertical red line is drawn midway between his feet, and he obviously has more of his body mass left of that red line. However, that doesn't mean that he is weight-pressure loading his left foot more than his right foot at that stage of his early downswing.
In fact, that image of Kevin Streelman comes from this article - https://www.swingcatalyst.com/learning-center/articles/body-mass-and-pressure
Here is the original image, that I copied from that article.
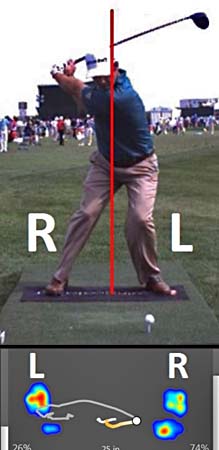
The Swing Catalyst COP-measurements can be seen below the image of Kevin
Streelman, and he has 74% of his overall-COP measurement under his right foot,
and only 26% of his overall COP-measurement under his left foot at that stage of
his early downswing. That "fact" shows that there is no correlation between
COM-measurements and COP-measurements and I don't think that a student-golfer
should even think of weight shift (COM-shift) when performing the early
downswing's rotary pelvic motion. If a student-golfer wants to perform the pro
golfer pattern of rotary pelvic motion during his early downswing, then he
should not think of shifting his body weight (shifting his COM) to his left foot
before he starts his rotary pelvic motion. He should simply think of performing
a centralised pivot motion between his feet while varying the COP-measurements
under his feet in the "correct" sequence (as previously described).
Question number 5:
If a golfer decides to use the pro golfer's pattern of rotary pelvic motion during his early downswing action, should he move the left knee targetwards before he starts to rotate his pelvis counterclockwise?
Answer:
Consider this animated gif of Bubba Watson's early downswing action.
![]()
If you look carefully, you will note that his lead knee moves targetwards before
he seemingly starts to rotate his pelvis clockwise. Does that mean that he activated the
lateral rotator muscles in his lead buttocks (which causes external rotation of
the lead femur) before he activated the lateral pelvic rotator muscles in his
trailing buttocks (which cause a clockwise rotation of his pelvis away from his
"stabilised" trailing leg)?
The answer is not necessarily! If a golfer decides to rotate his pelvis at the start of the downswing by activating both his lead and trailing lateral pelvic rotator group of muscles at the same time, then it would not be surprising to see the lead knee moving targetwards first because it doesn't take much muscle force to externally rotate the lead femoral head in the lead hip joint if the lead leg/foot is not weight-pressure loaded. By contrast, the trailing lateral pelvic rotator muscles have to build-up a finite level of isometric muscle contractile force before they can cause the pelvis to rotate away from the weight-pressure loaded ("stabilised") trailing leg, so there may be finite delay before the pelvis starts to rotate towards the target. A second biomechanical factor that may play a significant role is the degree of adduction of the lead thigh at the P4 position. If the lead thigh is significantly adducted at the P4 position (as seen in those four golfers from a bygone era), then it is not surprising that one would see overt evidence of the lead knee moving targetwards at the start of their downswing. By contrast, if you look at those four modern-day golfers (Jason Day, Jordan Spieth, Rory McIlroy and Adam Scott) at their end-backswing position, you will note that their lead thigh is not adducted and there is a large degree of separation between their knees at the P4 position. Therefore, they do not have to externally rotate their lead femur by very much at the start of their downswing to get into a position of dual-ER of both thighs (representing the Sam Snead "sit-down" look) by the P5 position - so it is not surprising that one may often not observe any overt targetwards motion of their lead knee at the start of their downswing.
Another question that often comes up is the question as to whether the targetwards motion of the left knee at the start of the downswing should be regarded as a separate leg motion that can independently increase swing power.
The SOMAX group of golf instructors adopt that position - see this video presentation at https://www.youtube.com/watch?v=SwJM-eBnTb4
Starting at the 3:26 minute time point of the video, the SOMAX presenter likens the rotary motion of the golf swing to a five stage rocket.
The SOMAX presenter states that stage 1 is due to leg motion, and he compares Rory McIlroy to Bobby Jones, who has an overt targetwards motion of his lead knee at the start of his downswing. The * SOMAX presenter believes that the targetwards motion of the lead knee is an independent leg action that can independently increase swing power. However, I personally believe that he is wrong because the targetwards motion of the lead knee is really due to activation of a pelvic girdle muscle (lateral pelvic rotator muscles of the lead buttocks) and it can only result in external rotation and abduction of the lead femur in the lead hip joint. I cannot fathom how anyone can rationally argue that it is an independent leg action that can independently increase swing power!
(* I have discussed this SOMAX video presentation in much greater detail in topic number 8 (subtopic b) of this review paper )
Question number 6:
Can a golfer, who uses a left-loading pelvic motion technique that weight-pressure loads the left leg at the P4 position, use the lateral pelvic rotator muscles to rotate the pelvis counterclockwise during phase 1 of the "left hip clearing" action?
Answer:
No!
There are certain golf instructors (primarily the S&T golf instructors) who instruct their student-golfers to get 60-70% of their weight-pressure over their left leg/foot at their end-backswing position.
Consider these capture images copied from Mike Bennett/Andy Plummer's Stack & Tilt DVD 2.0.
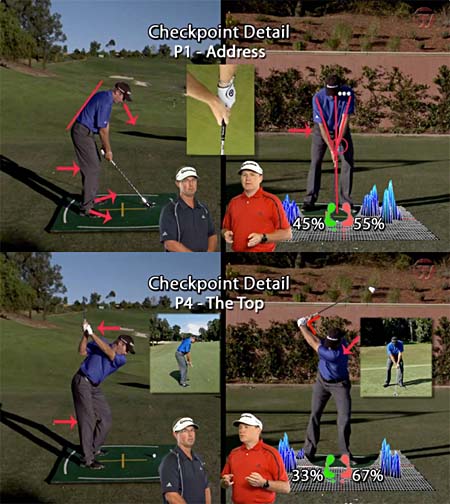
At address, the S&T golf instructors want their student-golfer to have 55% of his weight over his left foot and 45% over his right foot.
At the end-backswing position, the S&T golf instructors want the student-golfer to have 67% of his *weight over the left foot and 33% over the right foot.
( * The S&T golf instructors [Mike Bennett and Andy Plummer] are very vague and imprecise about differentiating between "weight" versus "weight-pressure loading", which is really represented by the COP-measurement under each foot - see this critical analysis of the S&T golf instructors' imprecise measurements for much more detailed information).
What would happen if a S&T golfer really had 67% of his weight-pressure (COP-measurement) under his left foot and only 23% of his weight-pressure (COP-measurement) under his right foot at the start of the downswing? Under those circumstances, the S&T golfer could not use his right-sided lateral pelvic rotator muscles to rotate his pelvis counterclockwise away from his right leg/foot because he could not easily "stabilise" his right leg in the absence of significant weight-pressure loading. If he attempted to activate his left-sided lateral pelvic rotator muscles, they would theoretically induce a clockwise rotation of his pelvis away from his weight-pressure loaded left leg - which means that the pelvis would be induced to rotate away from the target, and not towards the target. In other words, that S&T golfer could not possibly use his lateral pelvic rotator muscles to rotate his pelvis counterclockwise - as routinely seen in golfers who use the pro golfer's pattern of rotary pelvic motion. Therefore, the S&T golfer would likely have to use the "butt tuck-under-the-spine" pelvic thrust motion that is routinely recommended by S&T golf instructors.
Here is a link to a video of David Wedzik performing a drill that clearly demonstrates the S&T pelvic thrust maneuver.
https://www.youtube.com/watch?v=F0qw0r7pDQU
In that drill, David Wedzik recommends keeping the head (and therefore upper swing center) back while thrusting the lower swing center (pelvis) forward in a targetwards direction. Note that the pelvic motion is not a "pure" rotary motion of the pelvis and it involves a lot of left-lateral pelvic shift that will get the outer border of the left pelvis outside the outer border of the left foot by impact.
Here is capture image from the video which shows David Wedzik demonstrating the "butt tuck-under-the-spine" type of pelvic thrust action.

David Wedzik is demonstrating the "butt tuck-under-the-spine" type of pelvic thrust
action where he thrusts his pelvis (and lower swing center) in a direction that
is right-of-the-target - while keeping his head (and upper swing center) back.
To perform that type of pelvic thrust action, he must be activating his right gluteus maximus muscle that extends the right hip joint and forces the right-side of the pelvis well forward in an exaggerated right hip thrusting-spinning manner.
Note that the outer border of his left pelvis must be well outside the outer border of the left foot at that demonstrated-position when using this S&T type of pelvic thrust maneuver.
Although the S&T pelvic thrust maneuver is a workable pelvic motion pattern for a S&T golfer's downswing action, I personally think that it is not a back-friendly pelvic motion pattern, and I personally much prefer the pro golfer's pattern of rotary pelvic motion (as described in great detail in this review paper).
VJ Trolio also describes a left-loading pelvic motion pattern in his book [5] that gets 80% of his weight-pressure over his left leg at his end-backswing position, and he therefore encounters the same biomechanical problems experienced by a S&T golfer when it comes to using the lateral pelvic rotator muscles at the start of the early downswing - and I have described this particular problem-issue in great detail in topic number 2 of this review paper.
Question number 7:
What causes a golfer to perform a "goat humping" type of pelvic motion (also known as an "early extension" type of pelvic motion) during his downswing action?
Answer:
Consider these capture images of an anonymous golfer performing a "goat humping" type of pelvic motion during his downswing action.

Image 1 shows the anonymous golfer at his end-backswing position. Note that I
have drawn a red line against the back of his right buttocks and it represents
the tush line.
Image 2 shows how the golfer thrusts his right pelvis outward (towards the ball-target line) by activating his right gluteus maximus muscle that extends the right hip joint and "tucks-the-butt-under-the-spine" - thereby producing posterior pelvic tilt and a loss of spine bend inclination angle called "early extension". Note that the process of "early extension" continues throughout the remainder of the downswing so that he ends up with a "standing-up" posture at impact. The main difference, when compared to the S&T type of pelvic thrust action, is that this anonymous golfer is thrusting his pelvis outwards in the direction of the ball-target line while a S&T golfer thrusts his pelvis in a direction that is more right-of-the-target. That directional difference suggests that the anonymous golfer is also activating his left gluteus maximus muscle, so that both hip joints are symmetrically driven outwards in the direction of the ball-target line in such a manner that there is no rotation of the pelvis in the later downswing - note that the anonymous golfer's pelvis is square at impact (image 4).
What are the biomechanical differences in left femur motion and left foot motion during the late downswing/followthrough in a "front foot" golfer versus a "reverse foot" golfer (which I previously called a "reverse group" golfer)?
Answer:
I first came across the terms "front foot" golfer and "reverse group" golfer when I read Kevin Ball's PhD dissertation [6]. Kevin Ball studied a large number of golfers in his research study and he noted that were two distinct weight transfer styles during the downswing.
Here is the graph from his PhD dissertation [6].
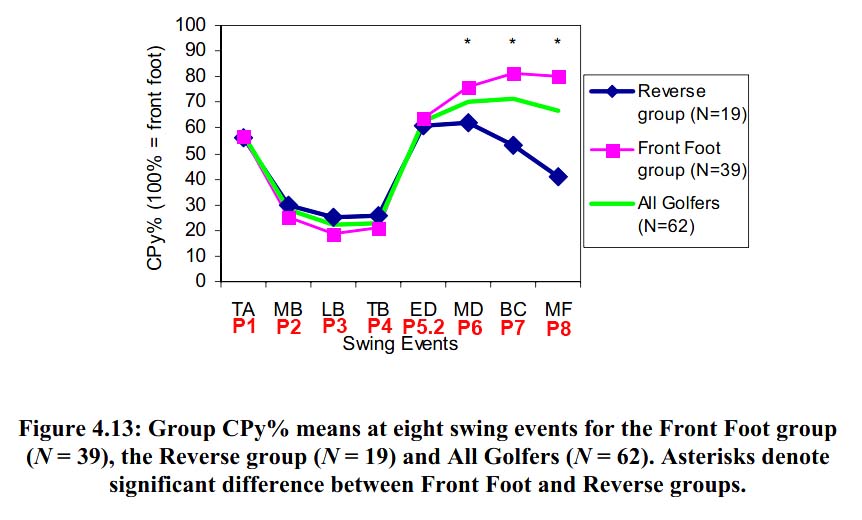
Note that he measured the COP under the front foot (expressed as percentage of
the overall COP measurement) at all time points during the golf swing - and I
have added P system time points on the X axis (in red) to make it easier for a
reader to interpret the graph.
Note that all the golfers have similar COP-measurements under the left foot at address (55% at P1), at the end-backswing position (~25% at P4) and at the P5.2 position (~60%). Note that the "front foot" golfers have 80% of their overall COP-measurement under their left foot at impact, while the "reverse group" golfers have only ~50% of their overall COP-measurement under their left foot at impact. That difference suggests that there is large difference in golf swing biomechanics happening in the later downswing (between P5.2 and P7) in "reverse group" golfers.
Kevin Ball was surprised by his findings and he couldn't explain why certain golfers were "reverse foot" golfers. I believe that "reverse foot" golfers are golfers (like Bubba Watson) who acquire a lot of secondary axis tilt and lateral bend during their later downswing and whose head is well back at impact and also during the early followthrough.
Consider these images of Bubba Watson at his P5 position and impact position.

Image 1 shows Bubba Watson at the P5 position (end of the hip-squaring phase).
Note that he has a small degree of of secondary axis tilt and very little
lateral bend.
Image 2 shows Bubba Watson at impact. Note that he has much more secondary axis tilt and lateral bend (curved yellow line). Note that his head is far back, and an imaginary line drawn vertically-down from his head (red arrowed line) will hit the ground just inside his trailing foot.
I strongly suspect that Bubba Watson is a "reverse foot" golfer, whose COP-measurement under the left foot is only ~50% of his overall COP-measurement at impact.
Consider Bubba Watson at the P8 position (images are from different swings)

Note that he still has a large amount of secondary axis and lateral bend, and
his head is well back.
Note that he seems to only have his lead forefoot grounded while his lead heel is free-floating - and note that his lead heel rotates inwards (away from the target) through impact. Also, note that his lead thigh is much more externally rotated (compared to a "front foot" golfer). I believe that his lead femur externally rotates much more than "average" because he is not weight-pressure loading his lead foot at impact (as seen in a "front foot" golfer) and that allows his actively contracting lead gluteus maximus muscle to more easily externally rotate his lead femur much more than the amount seen in a front foot golfer (who is weight-pressure loading his lead leg/foot at impact).
Note that his pelvis very open at impact/post-impact and that is likely due to the fact that the lead hip joint can more easily be pulled back (further away from the target) in a "reverse foot" golfer's late downswing secondary to the isotonic contraction of the lead gluteus maximus muscle - if the lead heel is "free-floating" and if the lead femur/leg can more easily externally rotate because the lead foot is not weight-pressure loaded.
Consider an example of a "front foot" golfer who has 77% of her overall COP-measurement under her left foot at impact - Suzann Pettersen.
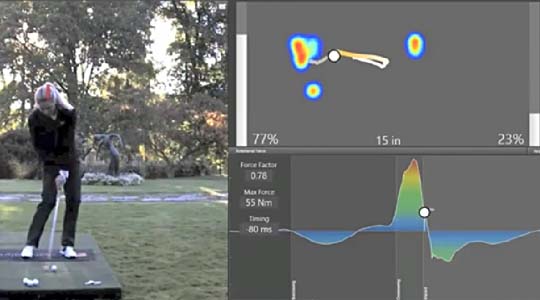
Note that Suzann Pettersen has very little secondary axis tilt/lateral bend at
impact.
Note that her left thigh is not externally rotated very much at impact and note that her left heel is well grounded and not spinning inwards.
Note that her pelvis is not very open at impact (compared to Bubba Watson) and that is likely due to the fact that it is biomechanically more difficult to externally rotate the left femur if it is more weight-pressure loaded at impact.
If a "front foot" golfer is generating a lot of external rotary torque with respect to the left femur at impact (due to the active contraction of the left gluteus maximus muscle), then it is much more likely that his left forefoot will spin counterclockwise (targetwards) as his left leg pivots counterclockwise around the axis point of his solidly grounded left heel (as seen in Gary Woodland's swing).
Capture images from a back-view video of Gary Woodland's swing.
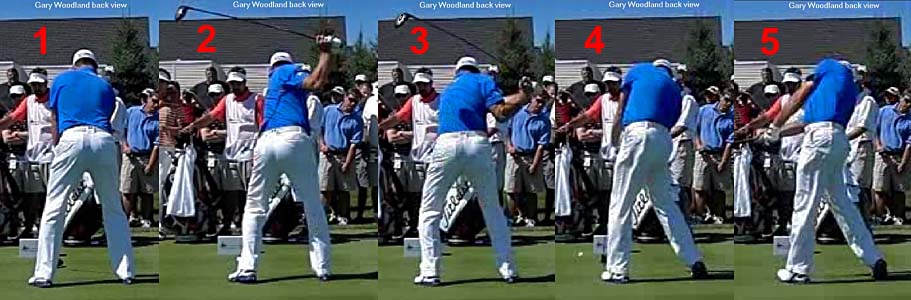
Image 4 shows Gary Woodland at impact, and image 5 shows him at the P8 position.
Note how he straightens his left leg, which is more vertical (compared to Bubba Watson's lead leg which is slanted more away from the target) and that is a characteristic feature of a "front foot" golfer. Note that he has far less secondary axis tilt than Bubba Watson at impact and at the P8 position, and his head is less far back. Note that he has less external rotation of his lead thigh at P8 when compared to Bubba Watson.
Note that his lead heel is solidly grounded, and that there is a small degree of left forefoot elevation off the gound as his left forefoot rotates externally to a very small degree.
If you are interested in reading much more about this topic - see topic number 13 in this review paper.
Jeffrey Mann.
February 2016.
References:
1. Electromyographic Analysis of the Hip and Knee During the Golf Swing. Bechler et al.
Abstract available at http://www.ncbi.nlm.nih.gov/pubmed/7670971
2. Ben Hogan's Five Lessons. Ben Hogan.

3. Swing Tips You Should Forget. Michael Jacobs.
4. The Anatomy of Greatness. Brandel Chamblee.
5. The Final Missing Piece of Ben Hogan's Secret Puzzle. VJ Trolio.
6. Weight Transfer Styles in The Golf Swing: Individual and Group
Analysis. Kevin Ball. (PhD thesis, Victoria University, Australia, 2006).
Available online at http://vuir.vu.edu.au/1432/1/Ball.pdf